This article provides a comprehensive guide to drafting a professional Neurology Seizure Disorder Consultation Letter. It explores essential clinical documentation, including seizure semiology, diagnostic findings, and personalized management plans to ensure seamless communication between specialists and primary care providers. Improve your clinical workflow and accuracy with our expert insights. Below are some ready to use templates.
Image cover: Neurology Consultation Report Templates and Samples for Seizure Disorders
Letter Samples List
- Initial Neurology Seizure Consultation Letter
- Primary Care Referral Acknowledgment Letter
- Post-Consultation Seizure Diagnosis Letter
- Electroencephalogram Test Results Notification Letter
- Antiepileptic Medication Treatment Plan Letter
- Seizure Pre-Consultation Patient Intake Letter
- Patient Driving Restriction Compliance Letter
- Neurology Seizure Follow-Up Appointment Letter
- Workplace Seizure Accommodation Clearance Letter
- Refractory Epilepsy Surgical Evaluation Letter
- Seizure Trigger And Lifestyle Management Letter
- Pediatric Seizure Disorder School Action Letter
- Discharge And Primary Care Transition Letter
Initial Neurology Seizure Consultation Letter
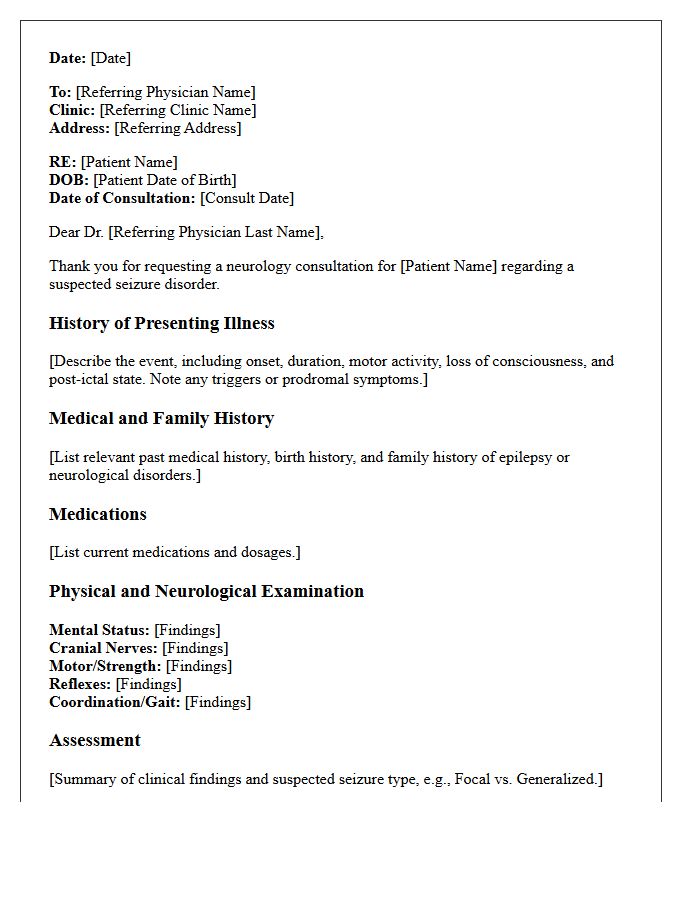
An initial neurology seizure consultation letter is a clinical document summarizing a patient's first specialist evaluation. It details the seizure semiology, potential triggers, and relevant family history to establish an accurate diagnosis. The letter outlines essential diagnostic investigations, such as EEG and MRI results, to classify seizure types. Furthermore, it specifies the management plan, including anti-seizure medication dosages and critical safety advice regarding driving or swimming. This communication ensures continuity of care between the neurologist and the primary care physician for optimal patient outcomes.
Primary Care Referral Acknowledgment Letter
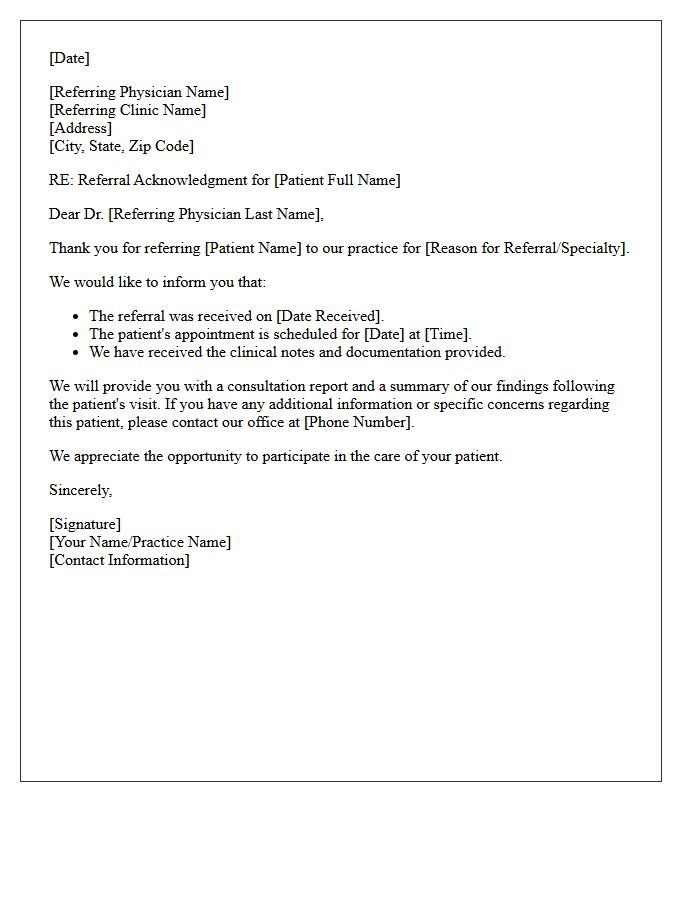
A Primary Care Referral Acknowledgment Letter is a formal document sent by a specialist to a primary care physician. It confirms the receipt of a patient referral and outlines the planned consultation or treatment timeline. This communication ensures continuity of care and verifies that the medical request is being processed. It serves as a vital record for patient tracking, professional accountability, and care coordination between healthcare providers to improve clinical outcomes and ensure no patient is lost in the system.
Post-Consultation Seizure Diagnosis Letter
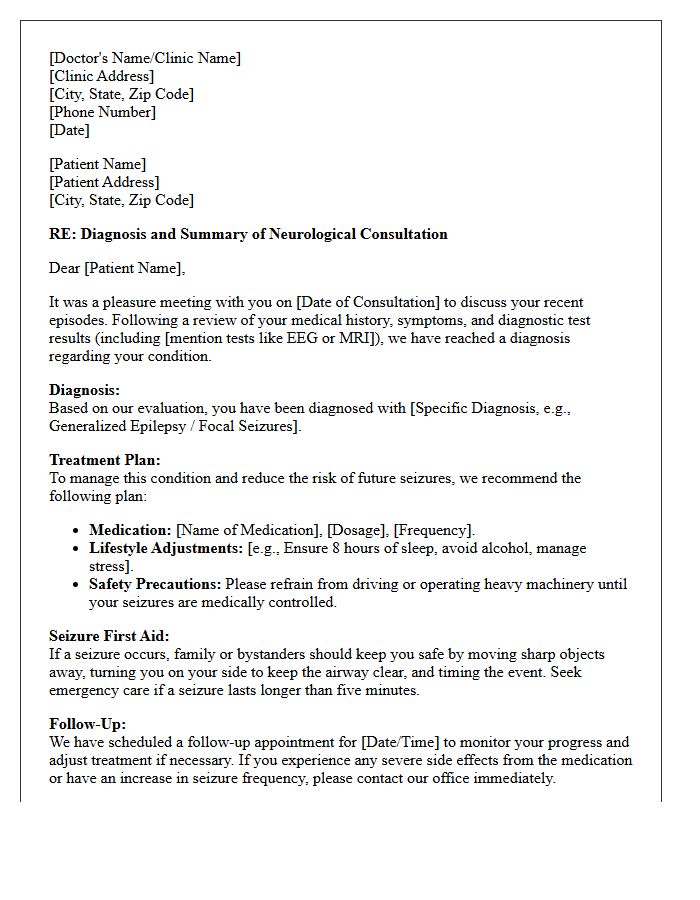
A post-consultation seizure diagnosis letter is a critical medical document confirming a clinical epilepsy diagnosis or seizure disorder. This formal record outlines the specific seizure type, recommended medication dosages, and potential triggers identified during evaluation. It serves as essential evidence for accessing specialized healthcare, securing workplace accommodations, and informing emergency responders. Patients should ensure the letter explicitly states safety restrictions, such as driving limitations, to maintain legal compliance and personal safety while managing their condition effectively within a structured treatment framework.
Electroencephalogram Test Results Notification Letter
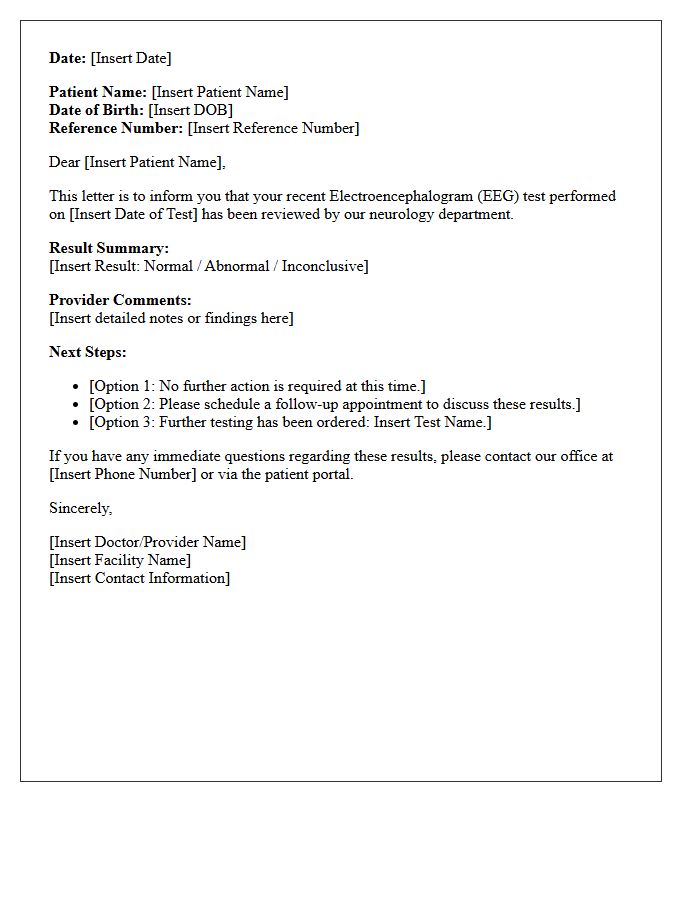
An Electroencephalogram (EEG) results notification letter informs you about the electrical activity recorded in your brain. It confirms if patterns are normal or show abnormalities like spikes or slowing, which may indicate seizures or other neurological conditions. While the letter provides a summary, it is essential to discuss the findings with your neurologist to understand the clinical significance. Always keep a copy for your medical records and follow any follow-up instructions or diagnostic recommendations provided by your healthcare provider to ensure proper treatment planning.
Antiepileptic Medication Treatment Plan Letter
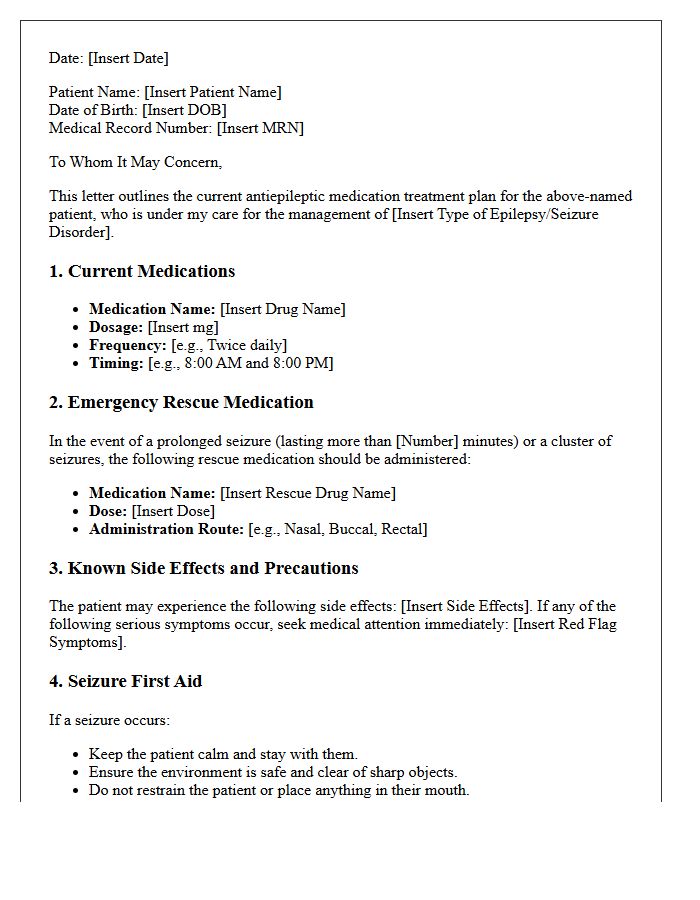
An Antiepileptic Medication Treatment Plan Letter is a critical medical document detailing a patient's specific drug regimen, dosages, and emergency protocols. It ensures continuity of care across healthcare providers and schools, minimizing the risk of medication errors. This formal record outlines seizure types, potential side effects, and clear instructions for rescue medication administration during prolonged episodes. Having this updated letter readily available is essential for patient safety, legal documentation, and effective seizure management in both clinical and community settings.
Seizure Pre-Consultation Patient Intake Letter
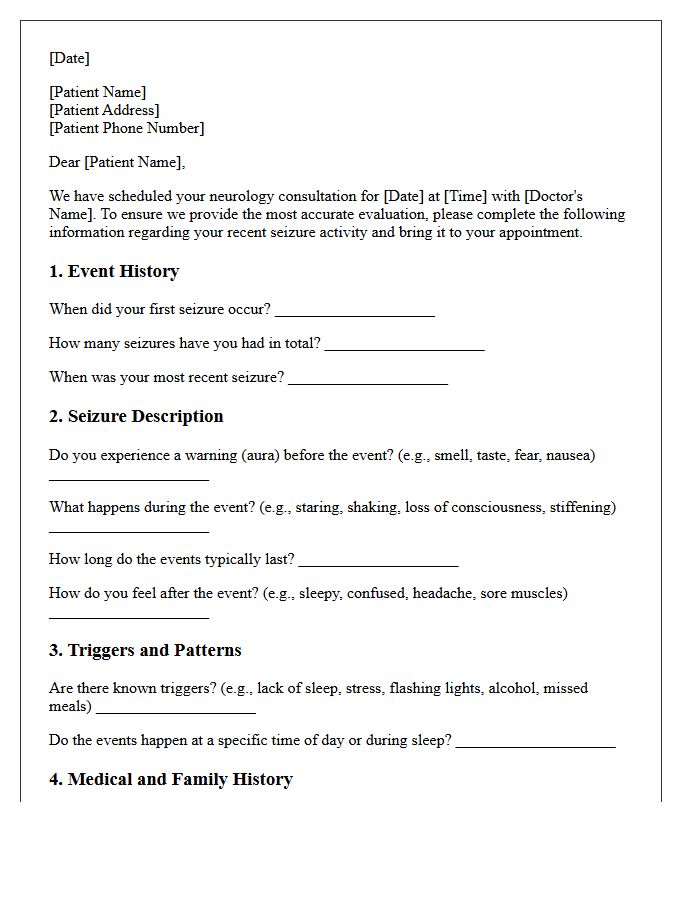
A Seizure Pre-Consultation Patient Intake Letter is a vital document used to gather detailed clinical history before meeting a specialist. It focuses on identifying seizure triggers, frequency, and specific physical symptoms experienced during events. Providing accurate information regarding medications and family history allows the neurologist to streamline the diagnostic process. Completing this intake thoroughly ensures a more productive appointment, helping the medical team develop an effective treatment plan tailored to the patient's specific neurological needs and safety concerns.
Patient Driving Restriction Compliance Letter
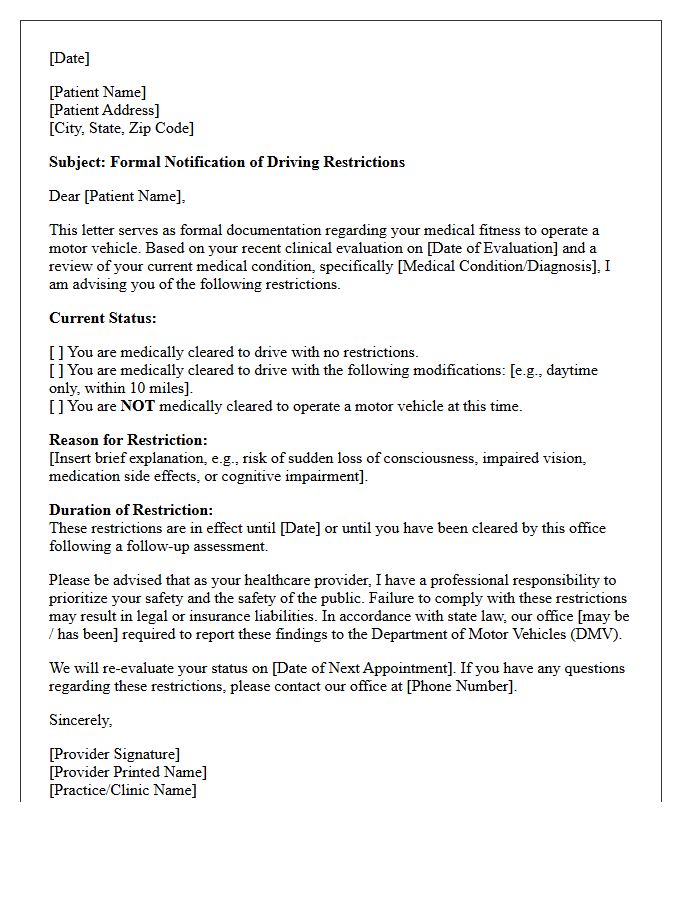
A Patient Driving Restriction Compliance Letter is a critical medical document confirming a patient's adherence to safety protocols following a diagnosis or surgery. It formally communicates that the individual is clinically fit to operate a motor vehicle or must remain restricted. This letter ensures legal and medical transparency, protecting both the patient and the public. Healthcare providers use it to document specific functional improvements or limitations, providing essential evidence for insurance companies, employers, or licensing authorities to verify that driving privileges align with current health status and safety standards.
Neurology Seizure Follow-Up Appointment Letter
A neurology seizure follow-up appointment letter is a vital document designed to evaluate treatment efficacy and patient safety. It typically requests a detailed seizure diary to track frequency, duration, and triggers since the last visit. The letter outlines necessary diagnostic tests, such as an EEG or MRI, and provides instructions for medication adjustments. Patients must bring a list of current prescriptions to ensure seizure control is optimized. This follow-up ensures personalized care and addresses any emerging side effects to improve overall neurological health and quality of life.
Workplace Seizure Accommodation Clearance Letter
A Workplace Seizure Accommodation Clearance Letter is a vital document from a healthcare provider confirming an employee's fitness for duty. It outlines specific functional limitations and necessary safety adjustments to ensure a productive environment. This letter protects legal rights under the ADA while helping employers implement reasonable accommodations, such as modified lighting or flexible schedules. Providing clear medical guidance minimizes workplace risks and ensures that individuals with epilepsy can perform their essential job functions safely and effectively without facing unfair discrimination or unnecessary safety hazards.
Refractory Epilepsy Surgical Evaluation Letter
A Refractory Epilepsy Surgical Evaluation Letter is a critical clinical document advocating for patients whose seizures remain uncontrolled by medications. It outlines the comprehensive diagnostic process, including Video-EEG monitoring, MRI, and neuropsychological testing, to pinpoint the seizure focus. This letter serves as a formal justification for neurosurgical intervention, such as resection or neuromodulation. By detailing the failure of anti-epileptic drugs and the impact on quality of life, it ensures medical necessity for insurance approval and specialized surgical care to achieve long-term seizure freedom.
Seizure Trigger And Lifestyle Management Letter
A Seizure Trigger and Lifestyle Management Letter is an essential medical document outlining specific factors that provoke seizures, such as sleep deprivation, stress, or flashing lights. It provides personalized protocols for caregivers, employers, or schools to minimize risks and ensure safety. By detailing lifestyle modifications and emergency contact information, this letter fosters a supportive environment. It serves as a vital tool for seizure prevention and helps medical professionals tailor treatment plans while empowering patients to manage their neurological health effectively through clear, documented guidance.
Pediatric Seizure Disorder School Action Letter
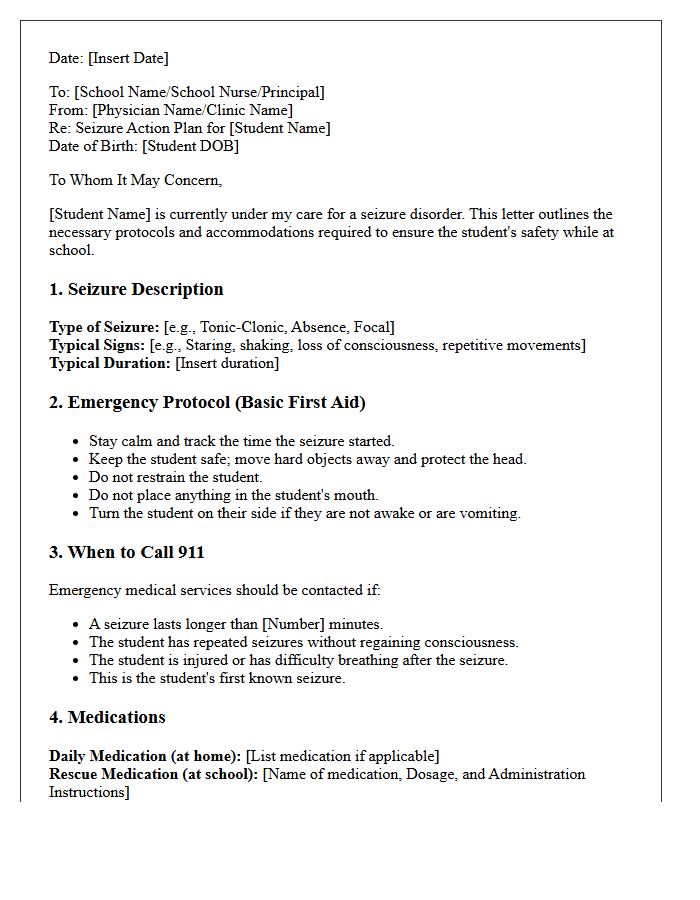
A Pediatric Seizure Disorder School Action Letter is a vital medical document ensuring student safety. It provides school staff with clear instructions on recognizing specific seizure types and administering emergency rescue medication. This Seizure Action Plan outlines necessary first aid steps, identifies triggers, and defines when to call emergency services. By formalizing communication between parents, neurologists, and educators, it creates a supportive environment that minimizes academic disruption while prioritizing the child's neurological health and immediate safety protocols during the school day.
Discharge And Primary Care Transition Letter
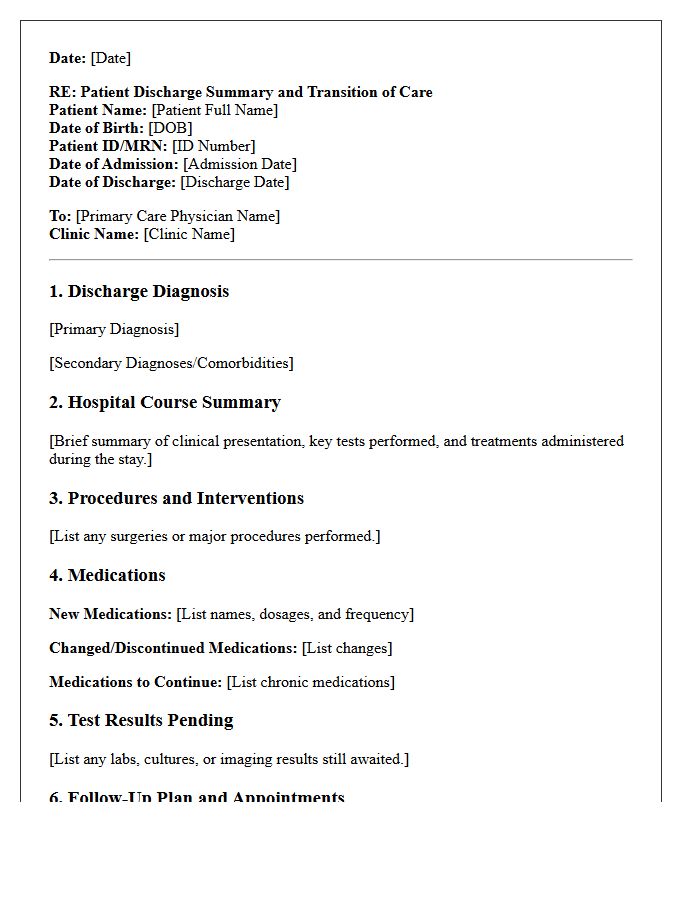
A Discharge and Primary Care Transition Letter is a vital clinical document ensuring continuity of care after hospital release. It provides the General Practitioner with essential data, including the primary diagnosis, medication changes, and pending test results. This communication minimizes medical errors and prevents avoidable readmissions. Patients should ensure their primary doctor receives this summary promptly to coordinate follow-up treatments and monitor recovery progress effectively. Accurate documentation during this transition phase is the cornerstone of safe and high-quality healthcare integration between secondary and community settings.
What information is included in a Neurology Seizure Disorder Consultation Letter?
A consultation letter typically includes the patient's clinical history, a detailed description of the seizure semiology, results from diagnostic tests like EEG or MRI, the neurologist's formal diagnosis, and a comprehensive management plan.
How does a neurologist differentiate between epilepsy and non-epileptic seizures in the report?
The neurologist uses a combination of witness accounts, video-EEG monitoring data, and clinical observations of the event's duration and characteristics to distinguish between epileptic seizures and psychogenic non-epileptic seizures (PNES).
What diagnostic codes are commonly used in seizure disorder consultation letters?
Neurologists typically utilize ICD-10 codes, such as G40 for various forms of epilepsy and recurrent seizures, to ensure accurate medical billing and standardized communication between healthcare providers.
Why is the "Plan of Care" section critical in a seizure consultation letter?
The Plan of Care outlines specific anti-epileptic drug (AED) dosages, titration schedules, safety precautions regarding driving and operating machinery, and emergency protocols for status epilepticus.
How can a primary care physician utilize the neurology consultation letter for ongoing management?
The letter serves as a clinical roadmap for the PCP to monitor medication side effects, coordinate follow-up laboratory work for therapeutic drug levels, and manage comorbid conditions while adhering to the specialist's recommendations.
Comments