Ensuring a smooth transition for elderly patients requires a comprehensive Geriatric Facility Transfer Discharge Letter. This essential document communicates critical medical histories, current medications, and care instructions to receiving providers to maintain patient safety and continuity of care. Proper documentation minimizes risks during facility changes and supports better health outcomes. Below are some ready to use template options to streamline your process.
Image cover: Essential Templates and Samples for Geriatric Facility Transfer Discharge Letters
Letter Samples List
- Standard Geriatric Facility Transfer Discharge Letter
- Urgent Medical Clinic Geriatric Facility Transfer Discharge Letter
- Memory Care Geriatric Facility Transfer Discharge Letter
- Skilled Nursing Geriatric Facility Transfer Discharge Letter
- Post-Acute Rehabilitation Geriatric Facility Transfer Discharge Letter
- Palliative Care Geriatric Facility Transfer Discharge Letter
- Long-Term Care Geriatric Facility Transfer Discharge Letter
- Hospice Geriatric Facility Transfer Discharge Letter
- Assisted Living Geriatric Facility Transfer Discharge Letter
- Cognitive Decline Geriatric Facility Transfer Discharge Letter
- Post-Surgical Geriatric Facility Transfer Discharge Letter
- Complex Care Geriatric Facility Transfer Discharge Letter
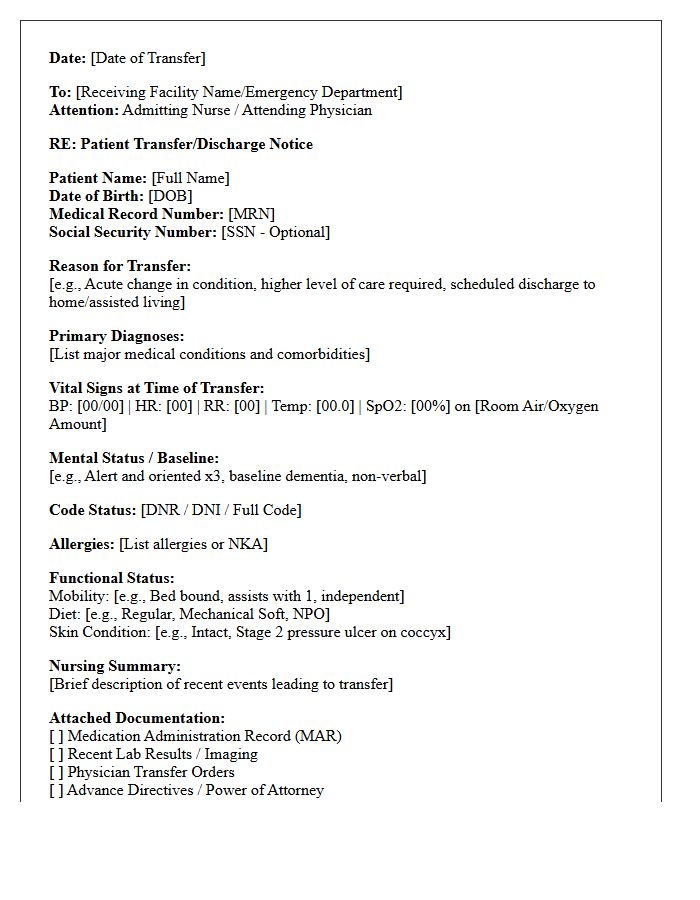
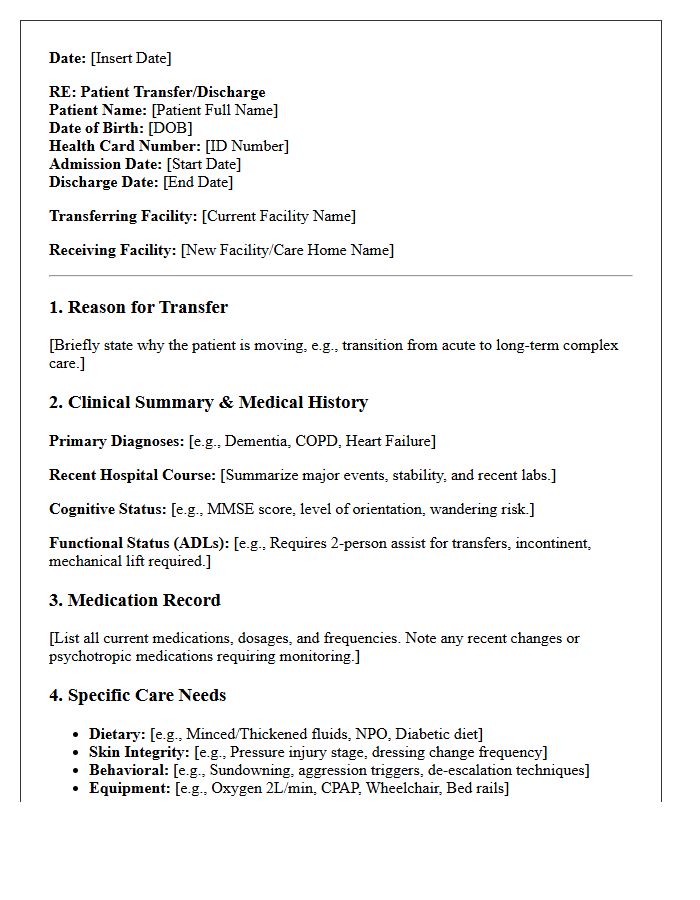
Standard Geriatric Facility Transfer Discharge Letter
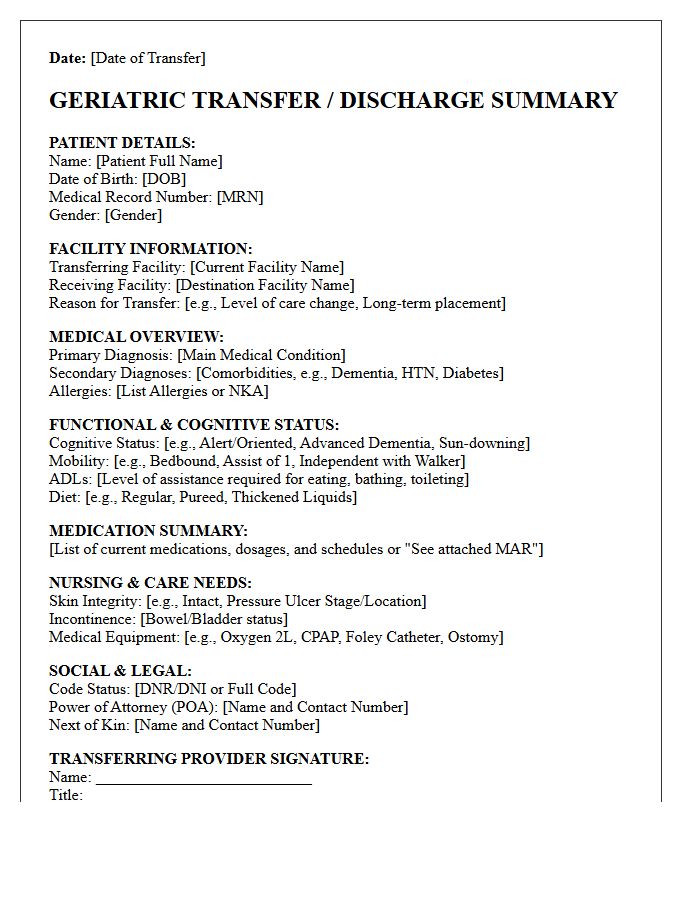
A Standard Geriatric Facility Transfer Discharge Letter is a vital clinical document ensuring seamless continuity of care. It must include a comprehensive medication administration record, recent vital signs, and the patient's baseline cognitive status. Clearly outlining the primary diagnosis and follow-up requirements prevents medical errors during transitions. Detailed communication regarding functional abilities and resuscitation status (DNR/DNI) protects patient autonomy. Providing this accurate summary to the receiving team minimizes readmission risks and ensures geriatric patients receive appropriate, safe, and person-centered treatment across different healthcare settings.
Urgent Medical Clinic Geriatric Facility Transfer Discharge Letter
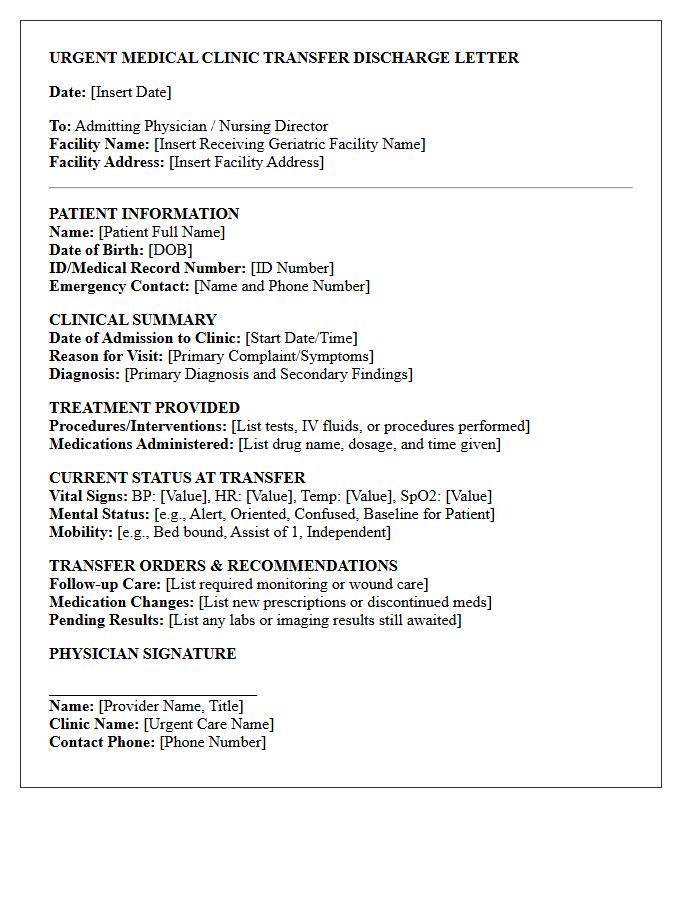
An urgent medical clinic geriatric facility transfer discharge letter is a critical communication tool ensuring continuity of care. It must provide a concise summary of the acute encounter, including vital signs, diagnostic results, and treatments administered. Key elements include the reason for transfer, current medication changes, and specific follow-up instructions for nursing staff. Accurate documentation prevents medication errors and potential rehospitalization, safeguarding the elderly patient's health during the transition back to their long-term care environment.
Memory Care Geriatric Facility Transfer Discharge Letter
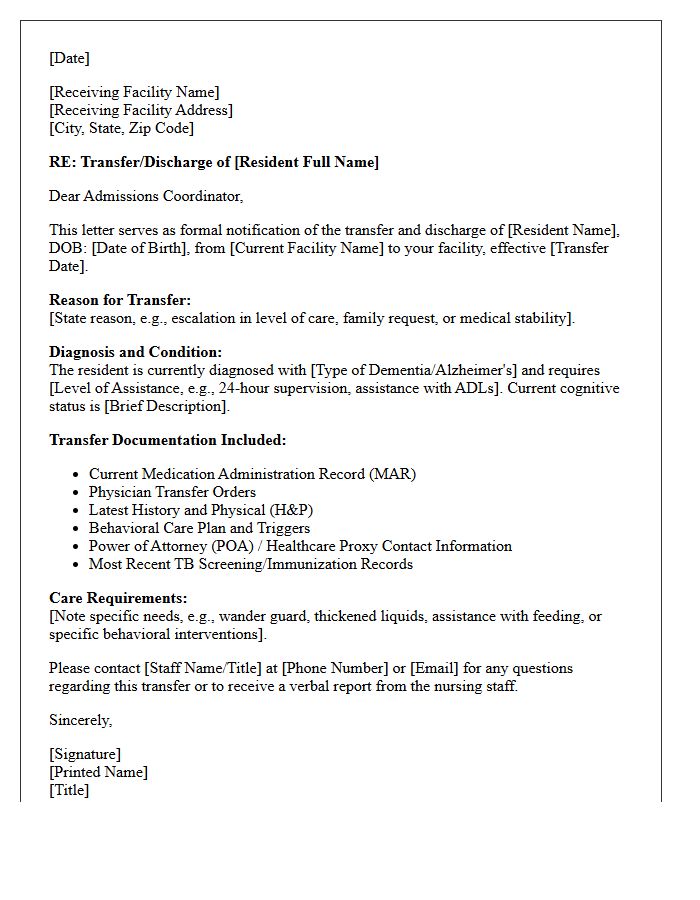
A Memory Care Geriatric Facility Transfer Discharge Letter is a critical clinical document ensuring safe patient transitions. It must summarize the patient's medical history, current medications, and specific behavioral patterns related to dementia. Clear communication regarding functional status and cognitive needs prevents lapses in care. This document serves as the primary tool for the receiving facility to maintain care continuity and manage potential risks effectively. Accurately detailing advanced directives and dietary requirements within the letter is essential for protecting the resident's health and dignity during the relocation process.
Skilled Nursing Geriatric Facility Transfer Discharge Letter
A Skilled Nursing Geriatric Facility Transfer Discharge Letter is a critical clinical document ensuring continuity of care during transitions. It must detail the patient's current medical status, active medications, and functional abilities. Essential components include the reason for transfer, comprehensive discharge instructions, and follow-up requirements. This document serves as a vital communication tool between healthcare providers to prevent medical errors and ensure patient safety. Accurate documentation of cognitive status and physical therapy needs is mandatory for a seamless handover to the receiving facility or home health agency.
Post-Acute Rehabilitation Geriatric Facility Transfer Discharge Letter
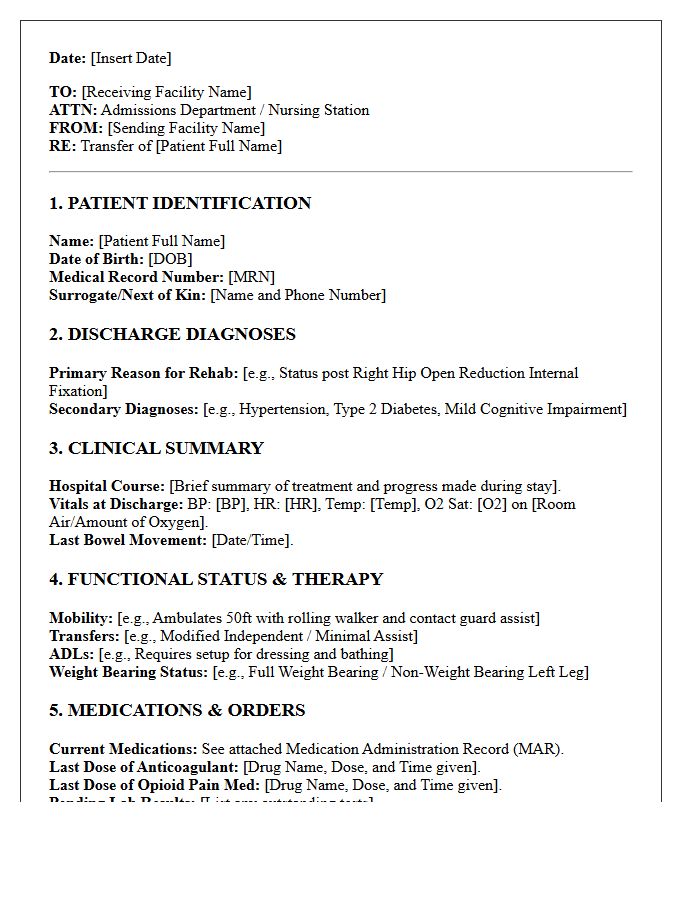
A post-acute discharge letter ensures a safe transition for elderly patients moving to a geriatric facility. It must include a comprehensive clinical summary, updated medication lists, and specific rehabilitation goals. Documenting functional status, cognitive levels, and pending follow-ups is critical to prevent readmission. This document serves as the primary communication tool between multidisciplinary teams, guaranteeing continuity of care. Accurate transfer information allows the receiving facility to implement immediate therapy protocols and nursing interventions tailored to the patient's recovery needs and physical limitations.
Palliative Care Geriatric Facility Transfer Discharge Letter
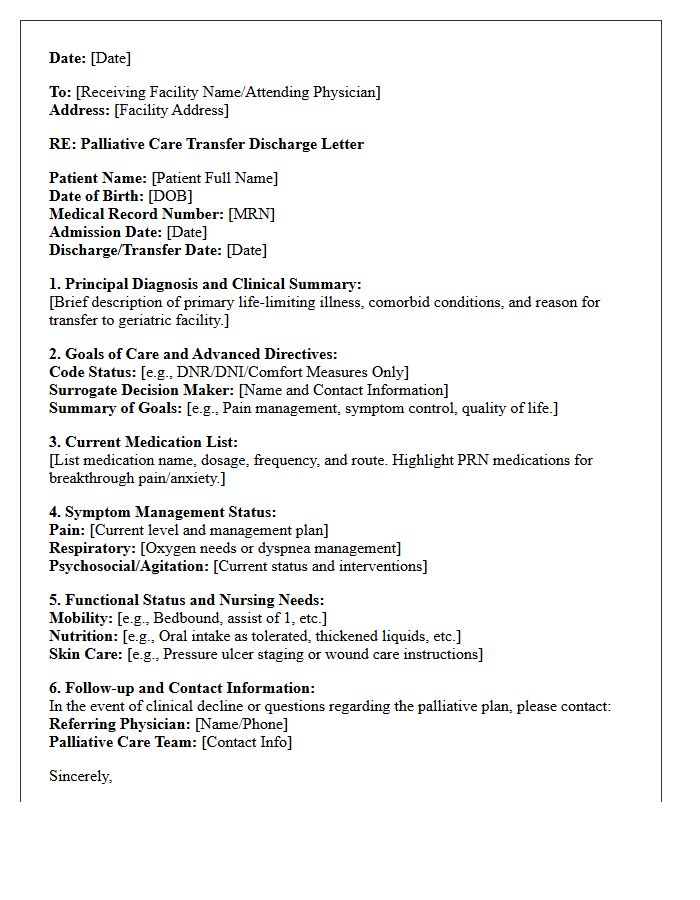
A Palliative Care Geriatric Facility Transfer Discharge Letter is a critical clinical document ensuring continuity of care for elderly patients. It must clearly communicate current symptoms, pain management protocols, and specific end-of-life preferences. Key components include updated medication lists, functional status, and advanced directives to prevent avoidable hospital readmissions. Accurate interdisciplinary notes help the receiving facility maintain the patient's comfort and dignity. Providing a detailed summary of palliative goals ensures that all healthcare providers align with the patient's physical, emotional, and spiritual needs during the transition process.
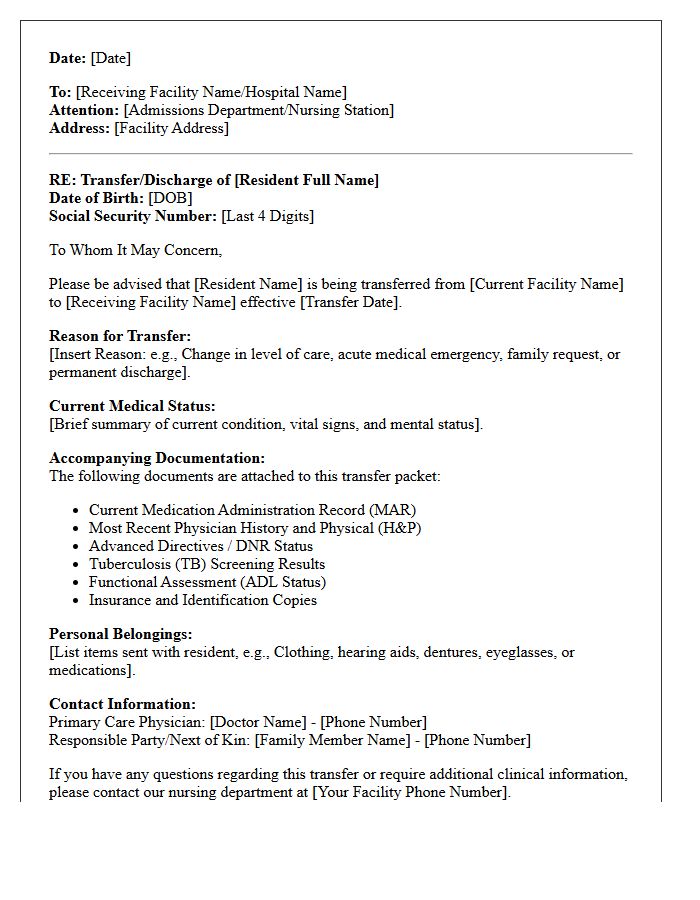
Long-Term Care Geriatric Facility Transfer Discharge Letter
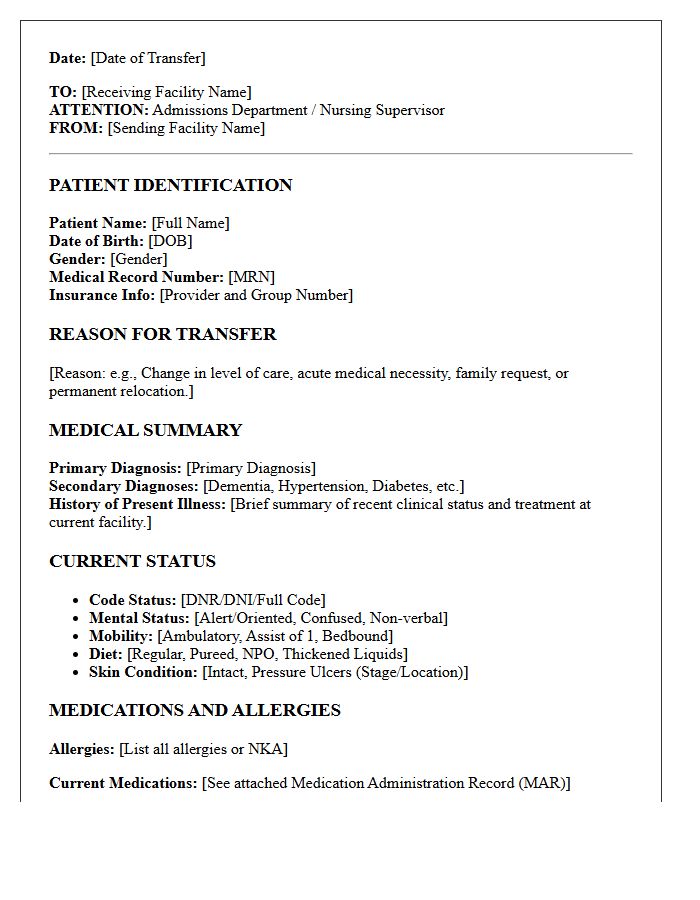
A Long-Term Care Geriatric Facility Transfer Discharge Letter is a vital clinical document ensuring continuity of care during transitions. It must detail the resident's current medical stability, comprehensive medication lists, and functional status. This formal record protects patient safety by communicating specific nursing needs and cognitive levels to the receiving provider. Proper documentation prevents medication errors and ensures that the individualized care plan remains uninterrupted. Under federal regulations, these letters also serve as legal notification regarding the resident's rights and the specific reason for the relocation or discharge.
Hospice Geriatric Facility Transfer Discharge Letter
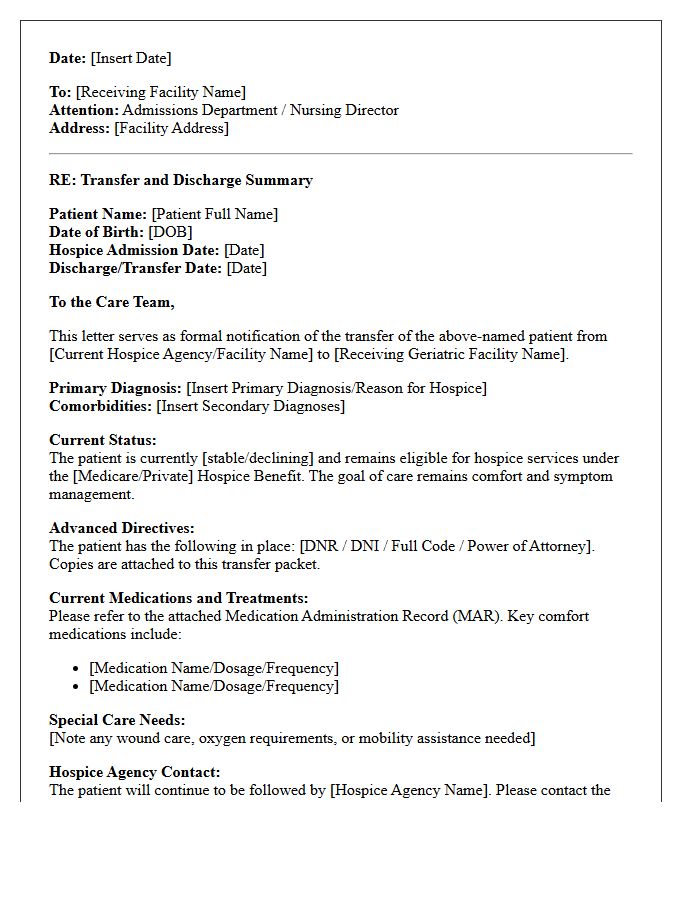
A Hospice Geriatric Facility Transfer Discharge Letter is a vital clinical document ensuring continuity of care during transitions. It summarizes the patient's medical history, current symptoms, and palliative goals. The primary focus is medication reconciliation and skin integrity reports to prevent errors. This record must clearly state the advance directives and comfort care protocols to guide the receiving facility's staff. Providing comprehensive details regarding pain management and functional status ensures a dignified, seamless handover, minimizing distress for elderly patients and their families during these critical end-of-life adjustments.
Assisted Living Geriatric Facility Transfer Discharge Letter
An Assisted Living Geriatric Facility Transfer Discharge Letter is a vital clinical document ensuring continuity of care. It must clearly outline the resident's current medical status, medication list, and functional abilities. The primary goal is to provide the receiving provider with essential health data to prevent complications during transitions. Key components include the reason for transfer, recent behavioral patterns, and advanced directives. This communication serves as a formal handoff, protecting patient safety and meeting regulatory compliance standards during the relocation process to a new care setting.
Cognitive Decline Geriatric Facility Transfer Discharge Letter
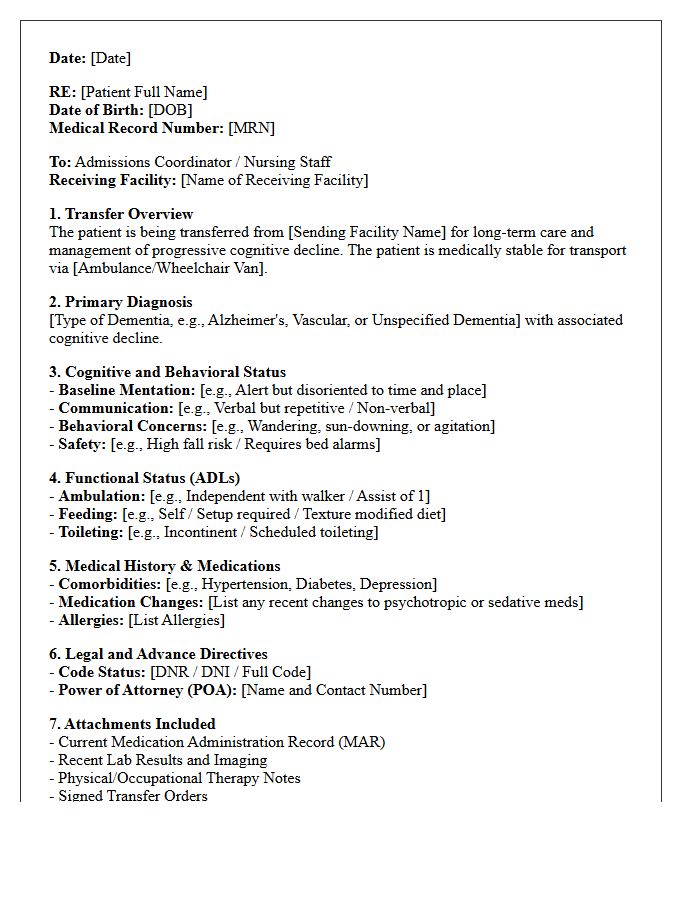
A geriatric discharge letter for facility transfer must prioritize the patient's cognitive status to ensure continuity of care. It is essential to document current functional abilities, behavioral patterns, and specific medication management needs. This semantic communication bridge prevents medical errors and assists the receiving facility in creating an appropriate person-centered care plan. Clear details regarding decision-making capacity and baseline mental health are vital for staff to monitor changes effectively and manage the progression of cognitive decline during the transition period.
Post-Surgical Geriatric Facility Transfer Discharge Letter
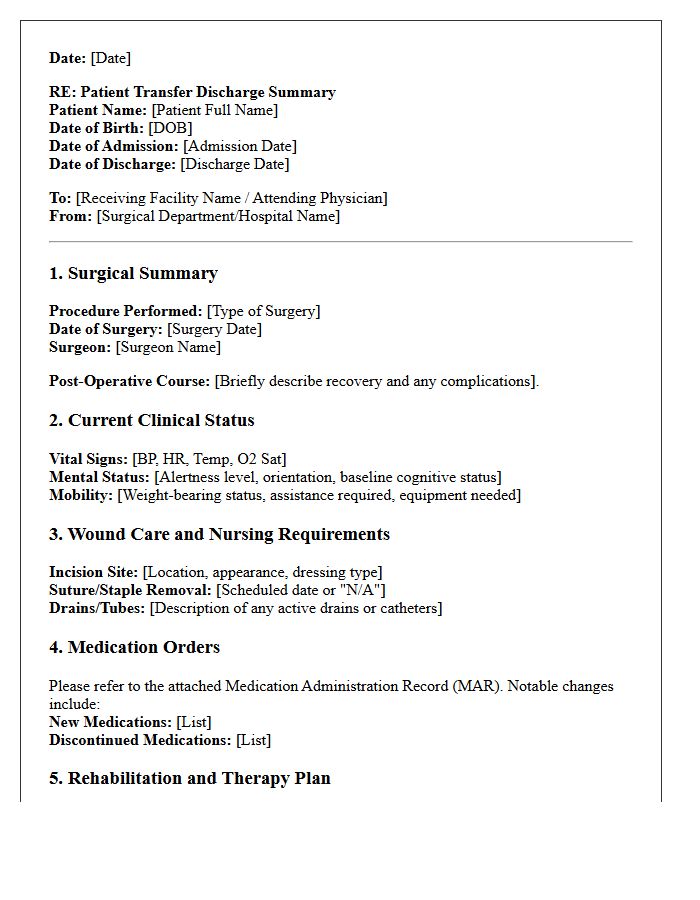
A post-surgical geriatric discharge letter is a critical communication tool that ensures a seamless transition to a skilled nursing facility. It must clearly outline the surgical procedure performed, anesthesia used, and the patient's current physiological stability. Key elements include an updated medication reconciliation, detailed wound care instructions, and specific mobility restrictions. This document minimizes medical errors by providing the receiving team with vital information regarding cognitive status, pain management protocols, and scheduled follow-up appointments, ultimately reducing the risk of hospital readmission for elderly patients.
Complex Care Geriatric Facility Transfer Discharge Letter
A Complex Care Geriatric Facility Transfer Discharge Letter is a critical clinical document ensuring safe transitions for elderly patients. It must contain an accurate medication profile, baseline cognitive status, and specific functional requirements to prevent readmissions. Key elements include the primary diagnosis, ongoing treatment plans, and follow-up appointments. This communication bridge minimizes medical errors by providing the receiving facility with a comprehensive summary of the patient's specialized needs. Precise documentation of care goals and recent laboratory results is essential for maintaining continuity and ensuring patient safety during the handoff process.
What is a geriatric facility transfer discharge letter?
A geriatric facility transfer discharge letter is a formal medical document that summarizes a senior patient's clinical history, current medications, and functional status to ensure a safe transition between care settings, such as from a hospital to a skilled nursing facility.
What essential information should be included in a geriatric transfer summary?
The letter must include the patient's primary diagnoses, recent test results, a reconciled medication list, cognitive status assessment, wound care instructions, and specific follow-up requirements for the receiving clinical team.
Why is a discharge letter critical for elderly patient safety?
It prevents medication errors, reduces the risk of hospital readmission, and ensures continuity of care by providing the receiving facility with a comprehensive roadmap of the patient's complex geriatric needs and baseline behaviors.
Who is responsible for preparing the transfer discharge documentation?
The discharging physician, hospitalist, or advanced practice provider is responsible for authoring the letter, often in coordination with a case manager or social worker to address social determinants of health and placement logistics.
How does a transfer letter address end-of-life or advance care planning?
The document should clearly state the patient's code status (DNR/DNI) and include copies of any legal directives, such as a POLST form or Power of Attorney, to ensure the patient's care preferences are honored at the new facility.
Comments