A Standard Patient Discharge Summary Letter is a vital clinical document ensuring continuity of care. It accurately communicates diagnosis, treatment received, and follow-up requirements between hospitals and primary care providers to enhance patient safety. Clear documentation reduces medication errors and prevents readmission during the transition home. To assist your clinical workflow, below are some ready to use templates.
Image cover: Effective Patient Discharge Summary Templates and Professional Letter Samples
Letter Samples List
- Standard General Patient Discharge Summary Letter
- Post-Surgical Clinic Patient Discharge Summary Letter
- Pediatric Care Patient Discharge Summary Letter
- Discharge Against Medical Advice Summary Letter
- Outpatient Physical Therapy Discharge Summary Letter
- Chronic Disease Management Discharge Summary Letter
- Psychiatric Clinic Patient Discharge Summary Letter
- Maternity and Obstetrics Patient Discharge Summary Letter
- Inter-Facility Transfer Patient Discharge Summary Letter
- Non-Compliant Patient Clinic Discharge Summary Letter
- Specialist Referral Patient Discharge Summary Letter
- Rehabilitation Center Patient Discharge Summary Letter
Standard General Patient Discharge Summary Letter
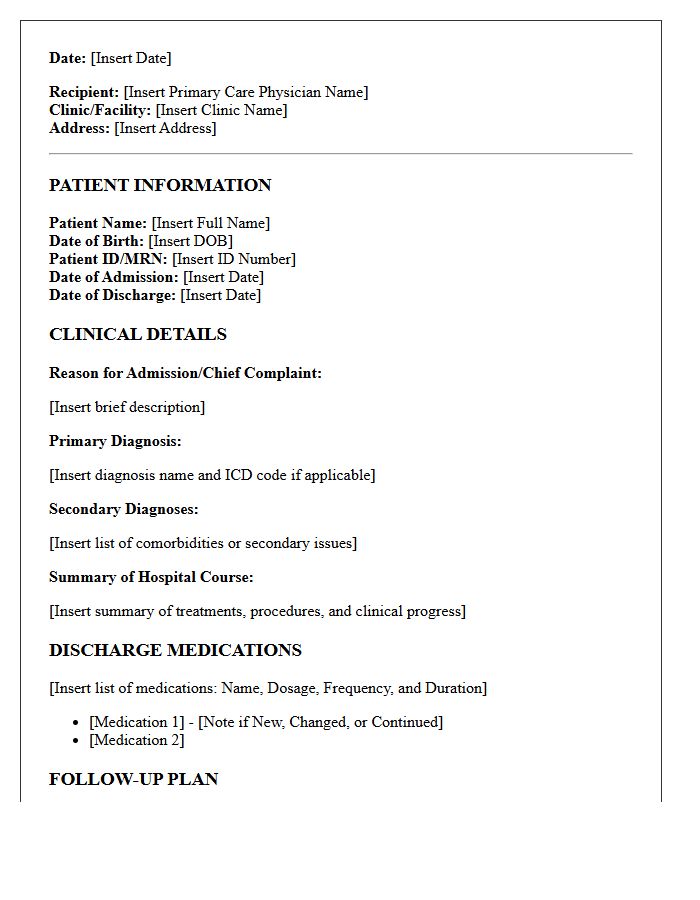
A Standard General Patient Discharge Summary Letter serves as the critical communication link between hospital care and primary providers. It must detail the clinical course, final diagnosis, and any medication changes to ensure patient safety. Key components include follow-up instructions and pending test results. This document is vital for continuity of care, helping general practitioners manage recovery effectively while preventing unnecessary readmissions. Accuracy in documenting procedures and post-discharge requirements ensures a seamless transition for the patient from acute settings back to their community healthcare team.
Post-Surgical Clinic Patient Discharge Summary Letter
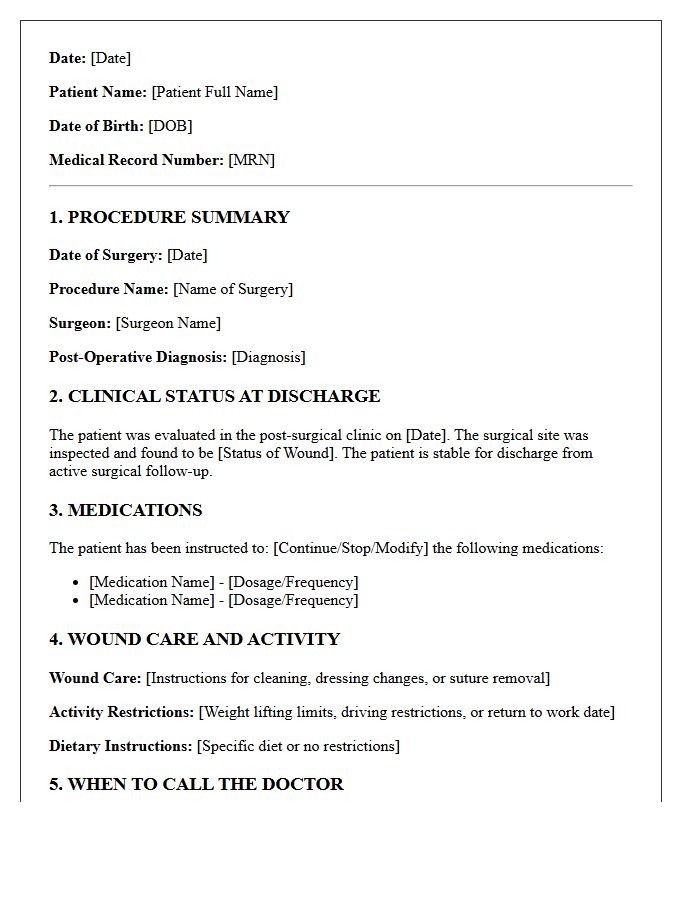
A post-surgical discharge summary is a critical medical document bridging hospital care and recovery. It outlines the surgical procedure performed, medication changes, and specific wound care protocols. Patients must prioritize the follow-up schedule to monitor healing progress effectively. Key sections include activity restrictions and a list of "red flag" symptoms requiring immediate intervention. This summary ensures continuity of care between specialists and primary physicians, empowering patients to manage their rehabilitation safely while reducing the risk of preventable readmissions through clear, actionable instructions.
Pediatric Care Patient Discharge Summary Letter
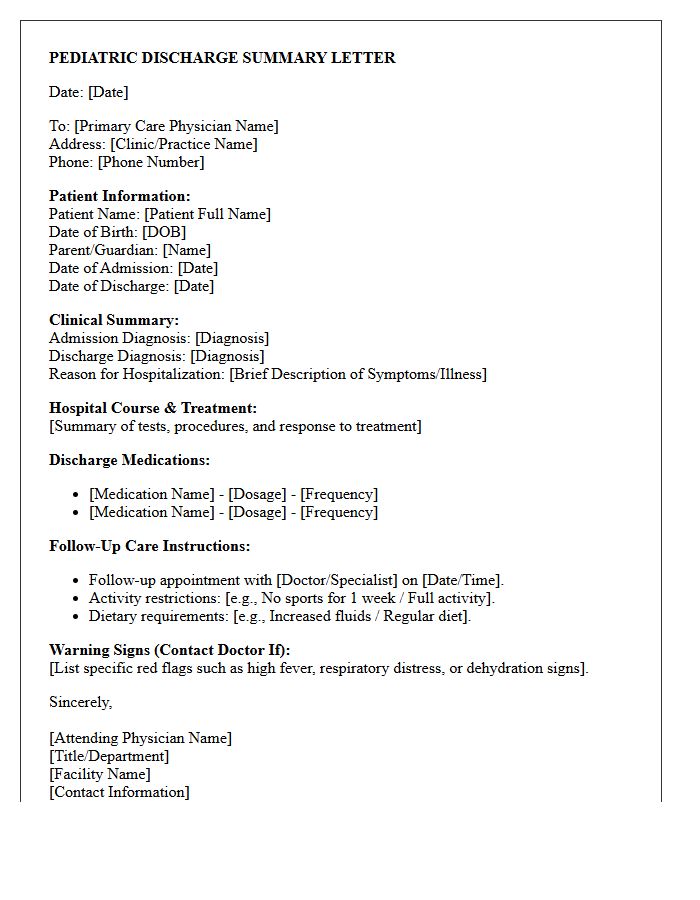
A Pediatric Care Patient Discharge Summary Letter is a vital clinical document that ensures a seamless transition of care from the hospital to the home setting. It must clearly outline the diagnosis, administered treatments, and required follow-up appointments to prevent readmission. For caregivers, understanding the specific medication dosages and emergency "red flag" symptoms is essential for recovery. This summary acts as the primary communication tool between hospital specialists and the child's primary pediatrician to maintain long-term health monitoring and patient safety.
Discharge Against Medical Advice Summary Letter
A Discharge Against Medical Advice (DAMA) summary letter is a vital legal document recording a patient's decision to leave healthcare facilities despite clinical warnings. It must clearly outline the specific risks, including potential disability or death, discussed during counseling. The letter documents the patient's mental capacity to refuse treatment and ensures a continuity of care plan is offered. For providers, this summary serves as critical malpractice protection by proving the informed refusal process was followed, while ensuring the patient remains eligible for future medical assistance without prejudice.
Outpatient Physical Therapy Discharge Summary Letter
An Outpatient Physical Therapy Discharge Summary Letter is a professional document that details a patient's clinical progress, functional outcomes, and final status at the conclusion of care. It serves as an essential communication tool for the referring physician to ensure continuity of treatment. Key components include the initial versus final range of motion, strength measurements, and achieved goals. This summary justifies the medical necessity of services provided and outlines necessary home exercise programs or follow-up recommendations to maintain long-term recovery and prevent future injury.
Chronic Disease Management Discharge Summary Letter
A Chronic Disease Management Discharge Summary Letter is a vital clinical document ensuring continuity of care during patient transitions. It provides primary physicians with essential data, including updated medication lists, diagnostic test results, and specific follow-up requirements. By summarizing inpatient interventions and long-term management goals, this letter minimizes medical errors and prevents avoidable readmissions. For patients with complex conditions, this communication serves as the definitive roadmap for ongoing treatment, ensuring that multidisciplinary healthcare teams remain aligned on the clinical pathway and therapeutic objectives post-discharge.
Psychiatric Clinic Patient Discharge Summary Letter
A Psychiatric Clinic Patient Discharge Summary Letter is a vital clinical document ensuring continuity of care after mental health treatment. It outlines the patient's diagnosis, medication regimen, and therapeutic progress during their stay. Crucially, it must include a detailed follow-up plan and comprehensive risk assessment to manage safety post-discharge. This summary facilitates seamless communication between the psychiatric facility and primary care providers, ensuring that ongoing support and rehabilitation goals are clearly communicated to prevent relapse and support long-term recovery.
Maternity and Obstetrics Patient Discharge Summary Letter
A maternity discharge summary is a vital medical document ensuring continuity of care after childbirth. It details the clinical course of delivery, neonatal outcomes, and specific medications prescribed. This record is essential for postpartum recovery tracking and must be shared with your primary physician or midwife. It highlights potential warning signs, follow-up appointment dates, and breastfeeding support. Having this summary ensures that any complications, such as hypertension or infection, are managed promptly by healthcare providers to protect the health of both mother and infant during the fourth trimester.
Inter-Facility Transfer Patient Discharge Summary Letter
An Inter-Facility Transfer Patient Discharge Summary Letter is a critical clinical document ensuring continuity of care during transitions. It summarizes the patient's diagnosis, medications, and treatments provided at the referring hospital. This record serves as a roadmap for the receiving facility, highlighting pending test results and required follow-up actions. Accurate documentation prevents medical errors, reduces readmission risks, and ensures the medical team has the necessary context to maintain patient safety and treatment efficacy during the transfer process.
Non-Compliant Patient Clinic Discharge Summary Letter
A Non-Compliant Patient Clinic Discharge Summary Letter serves as a formal notification ending the provider-patient relationship due to persistent treatment non-adherence. This document must clearly state the reason for termination, provide a specific effective date, and offer emergency care for a transitional period, typically thirty days. To mitigate legal liability and prevent claims of patient abandonment, the letter should include instructions for transferring medical records and recommendations for finding a new practitioner. Precise documentation of prior warnings ensures professional transparency and protects the clinic's regulatory standing.
Specialist Referral Patient Discharge Summary Letter
A specialist referral patient discharge summary letter is a critical communication tool that bridges the gap between secondary care and your primary physician. It provides a clinical overview of treatments, diagnostic results, and medication changes during specialist management. Ensuring accuracy in this document is vital for patient safety and continuity of care. It outlines specific follow-up instructions and ongoing management plans required for long-term health monitoring. Reviewing this summary helps patients understand their health status and ensures all healthcare providers remain aligned on the next steps of the recovery journey.
Rehabilitation Center Patient Discharge Summary Letter
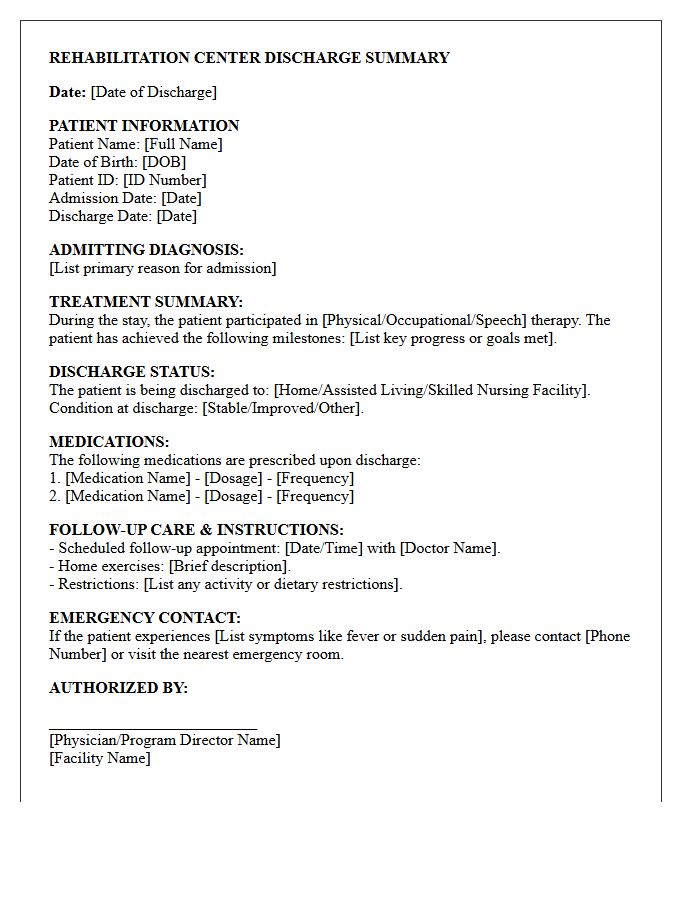
A Rehabilitation Center Patient Discharge Summary Letter is a vital clinical document ensuring safe transitions of care. It outlines the patient's functional progress, remaining deficits, and medication reconciliation details. This summary must include specific instructions for follow-up appointments and continued therapy requirements to prevent hospital readmission. By documenting the treatment outcomes and post-discharge care plan, it provides primary physicians and caregivers with the necessary roadmap to maintain the patient's recovery trajectory and long-term health stability outside the clinical setting.
What is a Standard Patient Discharge Summary Letter?
A Standard Patient Discharge Summary Letter is a clinical document provided to a patient and their primary care physician upon leaving a hospital. It outlines the diagnosis, treatment received, medications prescribed, and the necessary follow-up care required to ensure a safe transition from hospital to home.
Who is responsible for writing the patient discharge summary?
The discharge summary is typically authored by the attending physician or the medical team responsible for the patient's care during their hospital stay. It is reviewed and finalized before the patient is officially discharged to ensure all clinical information is accurate and complete for the next healthcare provider.
What key information is included in a discharge summary letter?
A comprehensive discharge summary includes the reason for admission, significant physical findings, results of diagnostic tests, procedures performed, a final diagnosis, and a detailed list of discharge medications. It also specifies activity restrictions, dietary requirements, and scheduled follow-up appointments.
Why is the discharge summary important for post-hospital care?
This document serves as the primary communication tool between hospital clinicians and outpatient providers. It prevents medical errors, such as medication duplication or missed follow-up tests, and ensures continuity of care, which significantly reduces the risk of hospital readmission.
How can patients access their discharge summary letter?
Patients are usually given a printed copy of the discharge summary at the time of their departure from the hospital. Additionally, many healthcare facilities upload a digital version to the patient's secure electronic health record (EHR) portal, where it can be viewed or downloaded by the patient and shared with other specialists.
Comments