A Letter of Medical Necessity is a critical document used to justify the clinical need for advanced diagnostic imaging, such as MRI or CT scans, to insurance providers. It outlines the patient's symptoms and previous treatments to secure prior authorization and ensure coverage. To help streamline your clinical documentation process, below are some ready to use templates.
Image cover: Effective Templates and Samples for Advanced Diagnostic Imaging Medical Necessity Letters
Letter Samples List
- Letter of Medical Necessity for Brain Magnetic Resonance Imaging with Contrast
- Letter of Medical Necessity for Computed Tomography Angiography of the Chest
- Letter of Medical Necessity for Positron Emission Tomography Scan in Oncology Staging
- Letter of Medical Necessity for High-Resolution Computed Tomography of the Lungs
- Letter of Medical Necessity for Cardiac Magnetic Resonance Imaging for Myocardial Viability
- Letter of Medical Necessity for Magnetic Resonance Imaging of the Lumbar Spine
- Letter of Medical Necessity for Functional Magnetic Resonance Imaging of the Brain
- Letter of Medical Necessity for Advanced Breast Magnetic Resonance Imaging
- Letter of Medical Necessity for Computed Tomography Enterography for Gastrointestinal Evaluation
- Letter of Medical Necessity for Nuclear Medicine Bone Scintigraphy
- Letter of Medical Necessity for Magnetic Resonance Arthrogram of the Shoulder Joint
- Letter of Medical Necessity for Coronary Computed Tomography Angiography Evaluation
- Letter of Medical Necessity for Whole Body Positron Emission Tomography
- Letter of Medical Necessity for Advanced Fetal Magnetic Resonance Imaging
- Letter of Medical Necessity for Multiparametric Magnetic Resonance Imaging of the Prostate
Letter of Medical Necessity for Brain Magnetic Resonance Imaging with Contrast
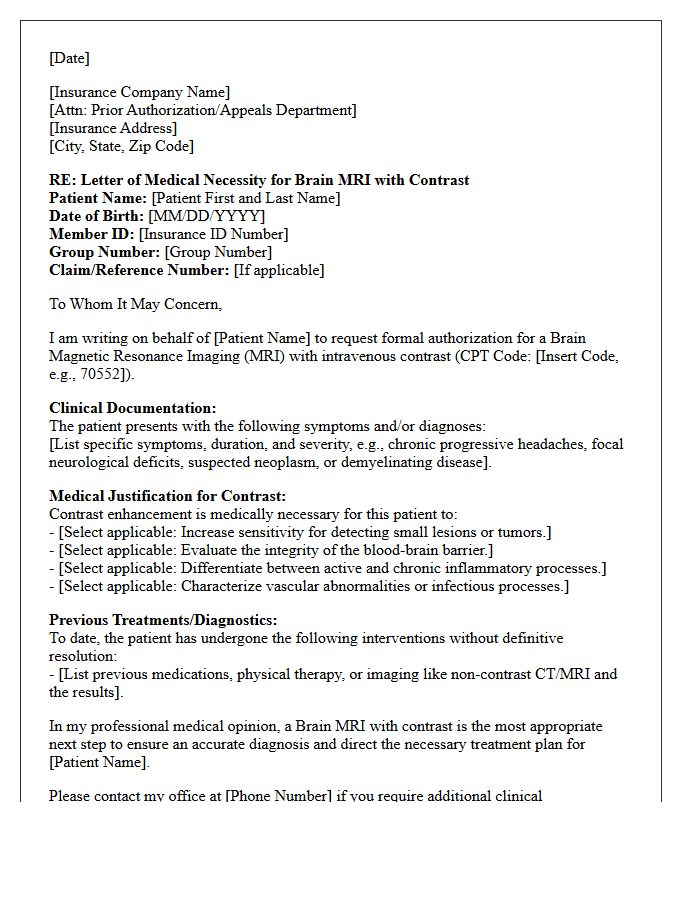
A Letter of Medical Necessity for a brain MRI with contrast justifies the clinical need for gadolinium to enhance diagnostic clarity. It must clearly outline the patient's specific symptoms, prior imaging results, and why non-contrast scans are insufficient. To secure insurance approval, the document should highlight how contrast helps differentiate between tumors, infections, or inflammatory lesions like multiple sclerosis. Providing detailed ICD-10 codes and a clear evidence-based rationale ensures the insurer understands why this advanced imaging is vital for an accurate diagnosis and subsequent treatment planning.
Letter of Medical Necessity for Computed Tomography Angiography of the Chest
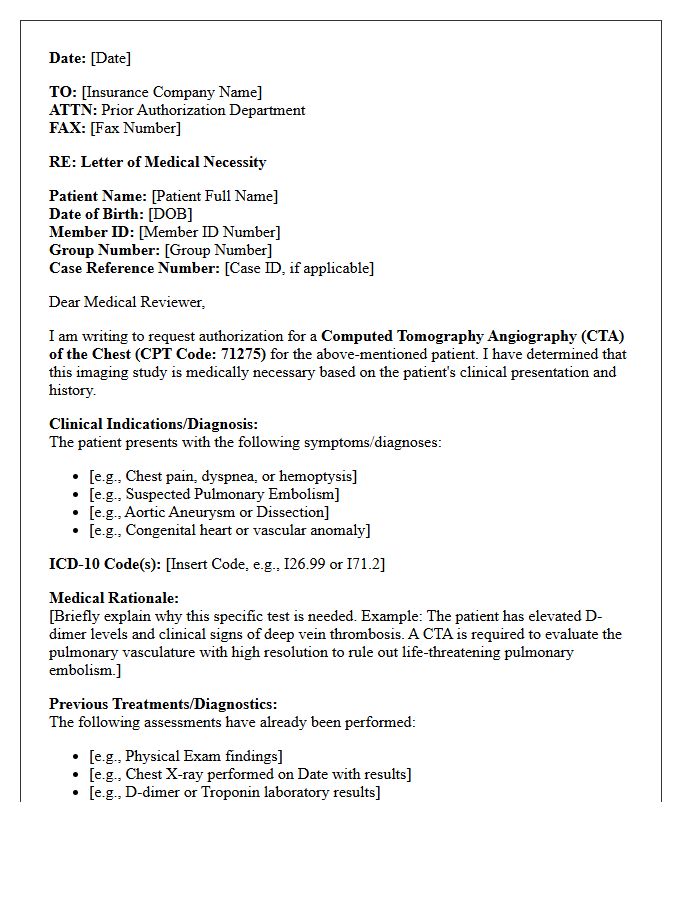
A Letter of Medical Necessity for a Chest Computed Tomography Angiography (CTA) is a critical document that justifies why this specialized imaging is essential for patient care. It must clearly outline the clinical indications, such as suspected pulmonary embolism, aortic aneurysm, or vascular anomalies, while documenting that standard tests were insufficient. To ensure insurance authorization, providers must include relevant symptoms, previous diagnostic results, and a specific ICD-10 code. This formal request bridges the gap between clinical needs and administrative approval, ensuring timely access to high-resolution cardiovascular diagnostics.
Letter of Medical Necessity for Positron Emission Tomography Scan in Oncology Staging
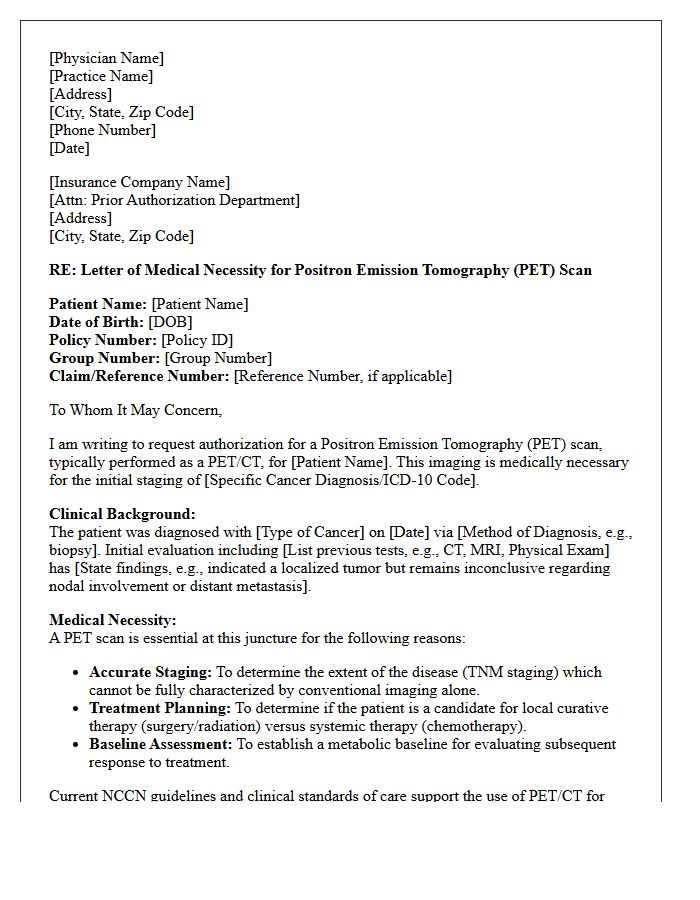
A Letter of Medical Necessity is essential for securing insurance coverage for a PET scan in oncology staging. It must provide detailed clinical justification, explaining why standard imaging is insufficient to determine the extent of cancer. The document should highlight how metabolic data will directly influence the treatment plan, such as clarifying nodal involvement or detecting distant metastasis. Clear documentation of the patient's diagnosis and the specific clinical indications ensures that the diagnostic procedure is recognized as medically indispensable for accurate staging and effective patient management.
Letter of Medical Necessity for High-Resolution Computed Tomography of the Lungs
A Letter of Medical Necessity is essential for insurance approval of a high-resolution computed tomography (HRCT) scan. It must clearly document the patient's clinical history, physical findings, and the diagnostic limitations of standard chest X-rays. Providers should emphasize specific symptoms, such as chronic dyspnea or suspected interstitial lung disease, to justify the need for superior anatomical detail. Including relevant ICD-10 codes and failed previous treatments ensures the request meets utilization management criteria, facilitating timely access to critical pulmonary imaging and effective treatment planning.
Letter of Medical Necessity for Cardiac Magnetic Resonance Imaging for Myocardial Viability
A Letter of Medical Necessity for cardiac MRI is essential to prove that assessment of myocardial viability is required for clinical decision-making. It must document the patient's history of ischemic cardiomyopathy or coronary artery disease. The letter justifies that Late Gadolinium Enhancement (LGE) imaging is the gold standard for distinguishing between scarred and hibernating tissue. This information is vital to determine if a patient will benefit from revascularization procedures, ultimately preventing unnecessary surgeries while ensuring optimal outcomes for those with recoverable heart function.
Letter of Medical Necessity for Magnetic Resonance Imaging of the Lumbar Spine
A Letter of Medical Necessity is a critical document used to justify why a patient requires an MRI of the lumbar spine. It outlines specific clinical indicators, such as chronic radiculopathy, neurological deficits, or failure of conservative treatments like physical therapy. Insurance providers require this detailed medical rationale to authorize coverage for the diagnostic scan. By documenting objective findings and correlating symptoms with suspected pathology, the physician proves the imaging is essential for guiding future treatment decisions and ensuring patient safety.
Letter of Medical Necessity for Functional Magnetic Resonance Imaging of the Brain
A Letter of Medical Necessity is a critical document required by insurance providers to justify Functional Magnetic Resonance Imaging (fMRI) of the brain. It must clearly outline the clinical indications, such as presurgical mapping of eloquent cortex or evaluating neurodegenerative diseases. The letter should detail how the procedure's results will directly influence treatment planning or surgical outcomes. Including specific ICD-10 codes and a summary of failed alternative diagnostics ensures the request meets the payer's criteria for medical necessity and improves the likelihood of coverage approval.
Letter of Medical Necessity for Advanced Breast Magnetic Resonance Imaging
A Letter of Medical Necessity is a critical document provided by a healthcare provider to justify the clinical need for Advanced Breast Magnetic Resonance Imaging. This document outlines specific risk factors, such as genetic mutations, dense breast tissue, or abnormal clinical findings, to advocate for insurance coverage. It bridges the gap between standard screening protocols and specialized diagnostics, ensuring patients receive precise supplemental screening when mammography is insufficient. For individuals at high risk, this letter is essential to secure approval for high-resolution imaging necessary for early cancer detection and comprehensive diagnostic evaluation.
Letter of Medical Necessity for Computed Tomography Enterography for Gastrointestinal Evaluation
A Letter of Medical Necessity is essential for insurance approval of a Computed Tomography Enterography (CTE). This document justifies why traditional imaging is insufficient for evaluating complex conditions like Crohn's disease or unexplained gastrointestinal bleeding. It must detail the patient's clinical history, symptoms, and previous failed treatments. By highlighting the unique ability of CTE to visualize small bowel pathology and transmural involvement, the letter ensures the medical necessity of the procedure is clear, reducing the likelihood of claim denials and facilitating timely diagnostic intervention.
Letter of Medical Necessity for Nuclear Medicine Bone Scintigraphy
A Letter of Medical Necessity is a critical document justifying why a patient requires Nuclear Medicine Bone Scintigraphy. It must detail the specific clinical indications, such as suspected fractures, bone metastases, or unexplained pain, that standard imaging cannot resolve. By outlining the patient's medical history and previous diagnostic failures, the provider proves the scan is essential for accurate diagnosis and treatment planning. This professional endorsement is vital for securing insurance prior authorization, ensuring the procedure is deemed medically appropriate and covered under the patient's specific healthcare policy.
Letter of Medical Necessity for Magnetic Resonance Arthrogram of the Shoulder Joint
A Letter of Medical Necessity is a critical document justifying why a standard MRI is insufficient for diagnosing specific shoulder pathologies. It highlights the clinical need for a Magnetic Resonance Arthrogram, which utilizes intra-articular contrast to enhance visualization of the labrum and rotator cuff tears. To ensure insurance approval, the letter must document previous failed conservative treatments, such as physical therapy, and specific physical exam findings. This formal justification bridges the gap between clinical symptoms and the specialized imaging required for accurate surgical planning or advanced diagnostic assessment.
Letter of Medical Necessity for Coronary Computed Tomography Angiography Evaluation
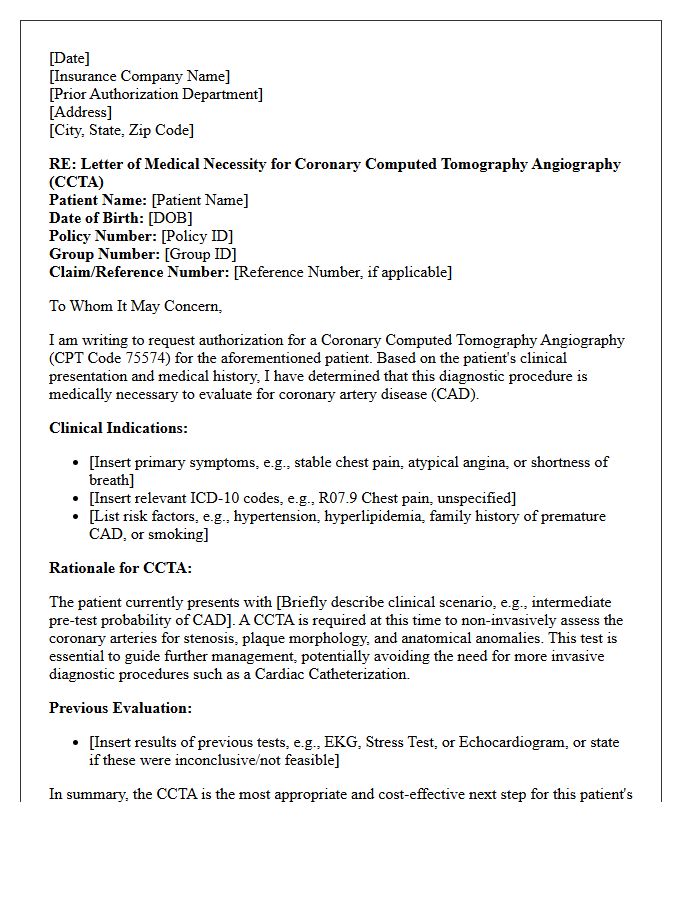
A Letter of Medical Necessity is essential for insurance coverage of a Coronary Computed Tomography Angiography (CCTA). It must demonstrate that the procedure is clinically required to evaluate symptoms like atypical chest pain or to screen high-risk patients. Providers must document why non-invasive imaging is superior to traditional stress tests for the specific case. Including relevant diagnostic codes and a detailed patient history helps justify the medical need, ensuring the CCTA evaluation is recognized as a vital tool for diagnosing coronary artery disease efficiently.
Letter of Medical Necessity for Whole Body Positron Emission Tomography
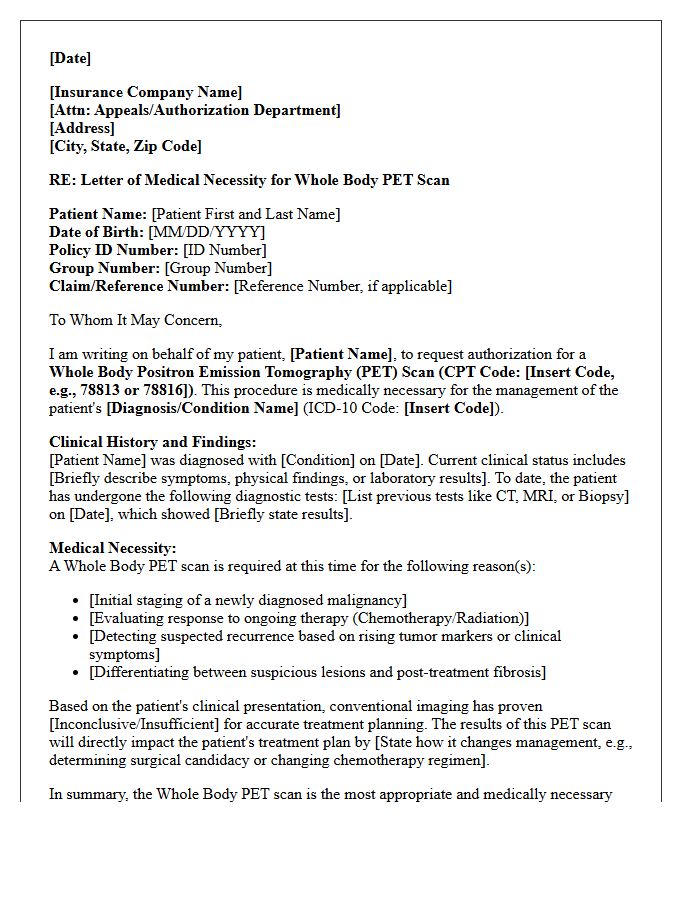
A Letter of Medical Necessity for a Whole Body Positron Emission Tomography (PET) scan is a critical document used to justify insurance coverage. It must clearly outline the patient's clinical history, diagnosis, and the specific reasons why a PET scan is superior to other imaging modalities. Physicians use this letter to demonstrate how the results will directly influence treatment planning, such as staging cancer or monitoring therapy response. Providing detailed medical evidence ensures that the diagnostic procedure is deemed medically necessary for optimal patient care outcomes.
Letter of Medical Necessity for Advanced Fetal Magnetic Resonance Imaging
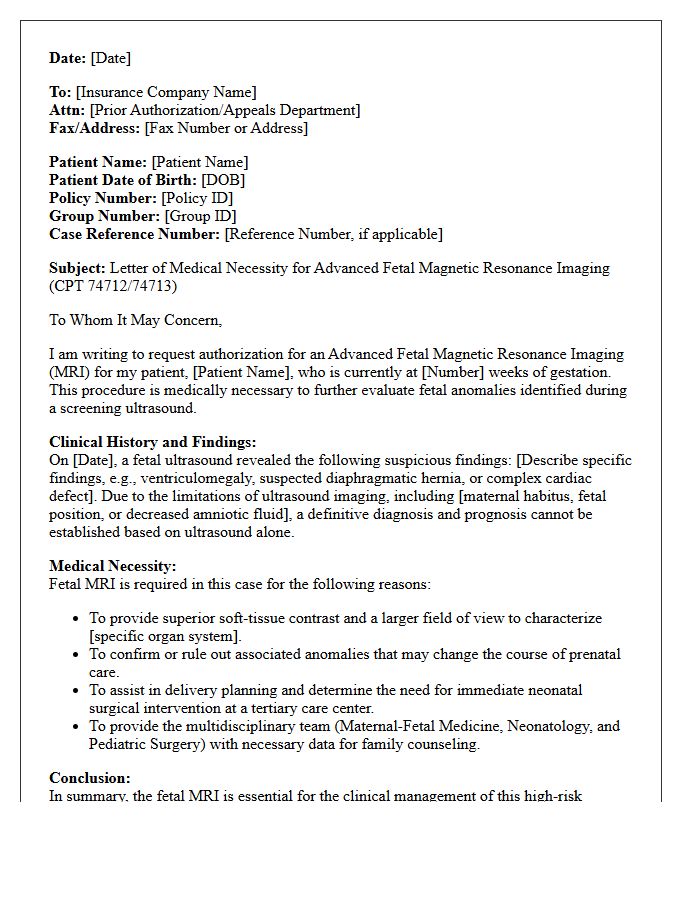
A Letter of Medical Necessity (LMN) is essential for insurance coverage of advanced fetal MRI. This document, written by a specialist, must prove the scan is clinically indispensable for diagnosing complex prenatal conditions that ultrasound cannot clearly resolve. It must detail how the Advanced Fetal Magnetic Resonance Imaging results will directly influence pregnancy management, surgical planning, or postnatal care. To avoid denials, the LMN should emphasize that the procedure is not elective but a critical diagnostic tool required to ensure the best possible outcomes for both the mother and the developing fetus.
Letter of Medical Necessity for Multiparametric Magnetic Resonance Imaging of the Prostate

A Letter of Medical Necessity (LMN) is essential for insurance coverage of a multiparametric MRI (mpMRI) of the prostate. It must clearly document clinical indications, such as an elevated PSA level, abnormal digital rectal exam, or the need for active surveillance. The document justifies why advanced imaging is superior to standard tests for detecting clinically significant cancer or guiding targeted biopsies. Providing detailed patient history and specific risk factors within the LMN minimizes claim denials and ensures timely access to precise diagnostic tools for effective prostate cancer management.
What is a Letter of Medical Necessity for advanced diagnostic imaging?
A Letter of Medical Necessity (LMN) is a formal document written by a healthcare provider that explains why a specific advanced imaging study, such as an MRI, CT scan, or PET scan, is clinically essential for a patient's diagnosis or treatment plan.
Why do insurance companies require a Letter of Medical Necessity for MRI or CT scans?
Insurance carriers require an LMN to verify that the requested advanced diagnostic imaging meets their specific clinical coverage criteria and to ensure the procedure is the most appropriate next step compared to lower-cost diagnostic alternatives.
What key elements should be included in an LMN for diagnostic imaging?
A comprehensive LMN should include the patient's clinical history, relevant symptoms, physical exam findings, previous treatments trialed (such as physical therapy or medications), and results of prior diagnostic tests like X-rays that justify the need for more advanced imaging.
How does a Letter of Medical Necessity assist in the prior authorization process?
The LMN serves as the primary evidence during the prior authorization process, providing the insurance medical reviewer with the clinical justification needed to approve coverage and minimize the risk of a claim denial or delay in care.
Can a patient write their own Letter of Medical Necessity for advanced imaging?
No, a Letter of Medical Necessity must be authored and signed by the ordering physician or a licensed healthcare provider, as it requires professional clinical judgment and an official medical signature to be valid for insurance review.
Comments