Properly managing long-term health requires organized documentation. A formal Request for Chronic Disease Management Records ensures you and your healthcare providers have access to vital treatment history, medication plans, and diagnostic trends. This article explains how to efficiently secure your clinical data to improve care coordination and health outcomes. To simplify the process, below are some ready to use template.
Image cover: Effective Templates and Samples for Chronic Disease Management Record Requests
Letter Samples List
- Request Letter for Diabetic Patient Medical Records
- Transfer Letter for Chronic Care Patient Records
- Specialist Referral Letter for Chronic Disease Records
- Patient Authorization Letter for Chronic Illness Records
- Insurance Verification Letter for Chronic Disease Management
- Primary Care Clinic Letter for Hypertension Treatment Records
- Care Coordination Letter for Chronic Disease History
- Ongoing Management Letter for Asthma Patient Records
- Post-Discharge Letter for Chronic Care Management Records
- Allied Health Request Letter for Chronic Disease Files
- Specialist Consultation Letter for Rheumatology Records
- Continuity of Care Letter for Chronic Illness Records
Request Letter for Diabetic Patient Medical Records
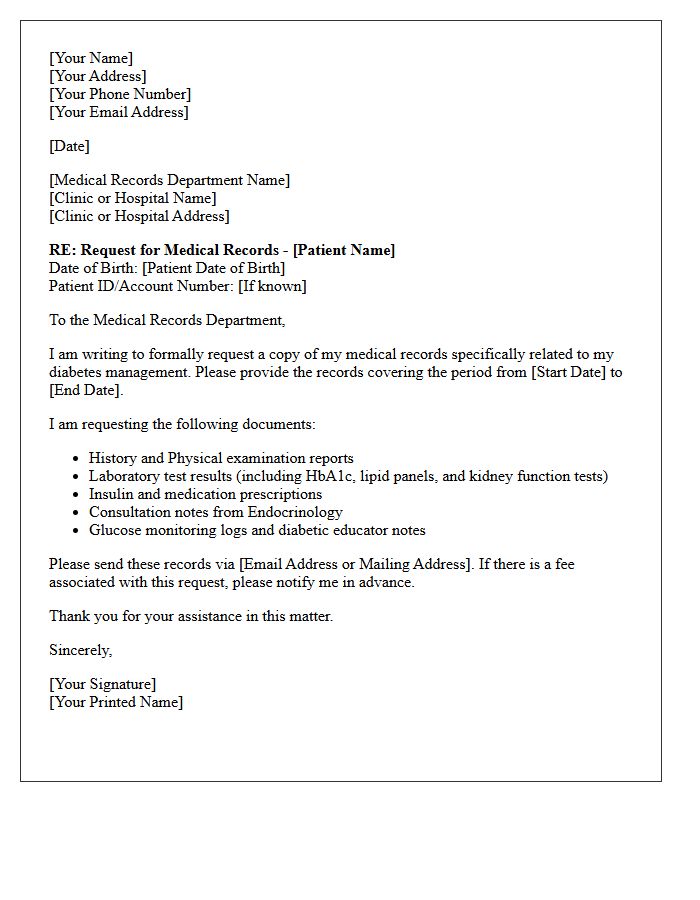
When drafting a request letter for a diabetic patient's medical records, it is essential to formally authorize the release of protected health information. Clearly state the patient's full name, date of birth, and specific dates of service required. Highlighting clinical documentation such as HbA1c results, insulin dosages, and glucose monitoring logs ensures a comprehensive overview for continuing care. Always include a signed HIPAA authorization to comply with privacy regulations. Providing a specific delivery method and a clear purpose for the request will help streamline the administrative process and prevent delays in medical management.
Transfer Letter for Chronic Care Patient Records
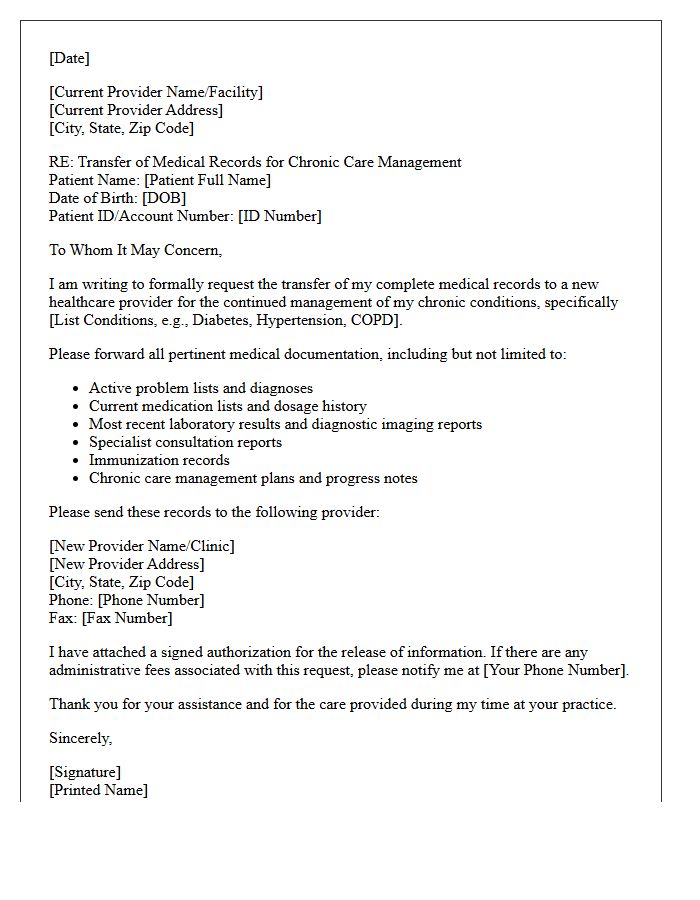
A Transfer Letter is a vital clinical document ensuring seamless continuity of care for chronic patients moving between providers. It must detail the current diagnosis, comprehensive medication lists, and ongoing treatment plans to prevent medical errors. Providing a clear medical history and recent lab results allows the new physician to manage long-term conditions effectively without diagnostic delays. This formal communication bridges the gap between healthcare settings, prioritizing patient safety and therapeutic stability during the transition of essential health records.
Specialist Referral Letter for Chronic Disease Records
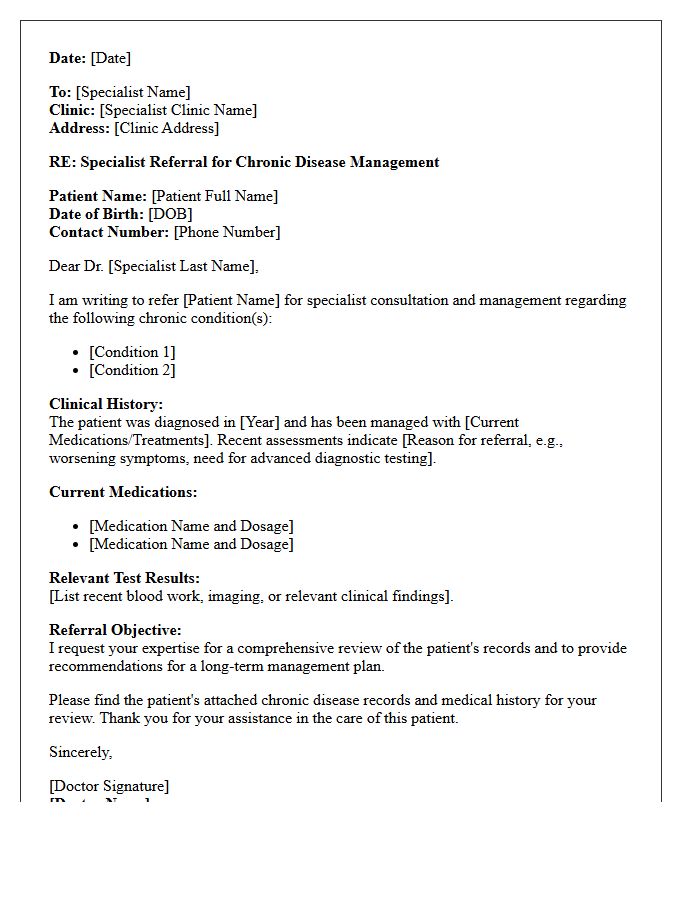
A specialist referral letter is a vital clinical document ensuring continuity of care for patients with long-term conditions. It provides the consultant with essential medical history, current symptoms, and specific diagnostic goals. For chronic disease management, this letter must include an accurate medication list and recent test results to prevent redundant evaluations. An effective referral facilitates multidisciplinary collaboration, ensuring your chronic disease records remain integrated across different healthcare providers for optimal treatment outcomes and streamlined insurance processing.
Patient Authorization Letter for Chronic Illness Records
A Patient Authorization Letter is a legal document granting healthcare providers permission to release sensitive medical history. When managing a chronic illness, this informed consent is essential for coordinating care between specialists, insurance companies, and caregivers. To ensure compliance with privacy laws like HIPAA, the letter must clearly specify the duration of access, the exact records being shared, and the designated recipients. Providing a detailed written authorization prevents delays in treatment and ensures that your entire medical team has the comprehensive data needed for effective long-term disease management.
Insurance Verification Letter for Chronic Disease Management
An Insurance Verification Letter is a critical document that confirms your policy covers long-term care for persistent health conditions. It details specific benefits, coverage limits, and pre-authorization requirements essential for managing a chronic illness. Obtaining this letter ensures that necessary treatments, medications, and specialist consultations are financially supported, preventing unexpected out-of-pocket costs. By validating your eligibility early, you secure a seamless continuum of care, allowing for effective healthcare planning and improved long-term clinical outcomes.
Primary Care Clinic Letter for Hypertension Treatment Records
A primary care clinic letter for hypertension treatment serves as a medical summary documenting your blood pressure history and medication efficacy. This document is essential for continuity of care between specialists and general practitioners. It outlines specific diagnostic results, lifestyle recommendations, and prescribed dosages to ensure patient safety. Having a formal record helps track long-term trends and prevents adverse drug interactions. Always ensure your letter includes your current treatment plan and most recent clinical readings to optimize your cardiovascular health management and support informed clinical decision-making during future appointments.
Care Coordination Letter for Chronic Disease History
A care coordination letter for chronic disease history is a vital medical document designed to facilitate seamless communication between healthcare providers. It provides a comprehensive summary of a patient's long-term conditions, current treatments, and diagnostic results. By ensuring all specialists have access to the same clinical data, it minimizes errors and prevents fragmented care. This collaborative tool is essential for maintaining continuity of care, optimizing treatment outcomes, and ensuring patient safety across diverse clinical settings through structured information exchange and clear management plans.
Ongoing Management Letter for Asthma Patient Records
The Ongoing Management Letter is a vital clinical document used to ensure continuity of care for asthma patients. It summarizes current symptom control, medication adherence, and lung function results. This record allows healthcare providers to track exacerbation frequency and adjust long-term treatment plans effectively. By maintaining an updated Asthma Action Plan within these records, clinicians can prevent emergency admissions and improve patient outcomes. Accurate documentation of triggers and inhaler technique ensures that every member of the care team remains informed about the patient's respiratory health status.
Post-Discharge Letter for Chronic Care Management Records
A post-discharge letter is a vital component of Chronic Care Management (CCM) records, ensuring seamless continuity of care. It serves as a clinical summary that bridges the gap between hospital treatment and outpatient monitoring. This document must detail medication changes, pending labs, and follow-up requirements to prevent readmissions. Accurate documentation within the patient's electronic health record is essential for meeting Medicare compliance standards and facilitating coordinated care transitions. Properly recorded letters allow healthcare providers to track recovery progress and manage complex chronic conditions effectively during the critical post-hospitalization period.
Allied Health Request Letter for Chronic Disease Files
An Allied Health Request Letter is a formal document used to coordinate specialized care for patients with chronic conditions. This request ensures that healthcare providers receive essential diagnostic data and patient history to develop effective treatment plans. To optimize outcomes, the letter must clearly state the clinical reasoning and specific services required under a Chronic Disease Management plan. Accurate documentation facilitates seamless communication between general practitioners and specialists, ensuring the patient remains eligible for Medicare rebates and receives integrated, high-quality multidisciplinary support for long-term health stabilization.
Specialist Consultation Letter for Rheumatology Records
A specialist consultation letter is a vital document summarizing a patient's rheumatology evaluation for chronic inflammatory conditions. It details physical findings, diagnostic results, and a long-term management plan tailored to autoimmune health. This record serves as the primary communication tool between the specialist and the primary care physician to ensure treatment continuity. Patients should maintain copies of these letters, as they provide an official history of disease activity and medication adjustments, which are essential for coordinating care and securing insurance approvals for complex biologic therapies.
Continuity of Care Letter for Chronic Illness Records
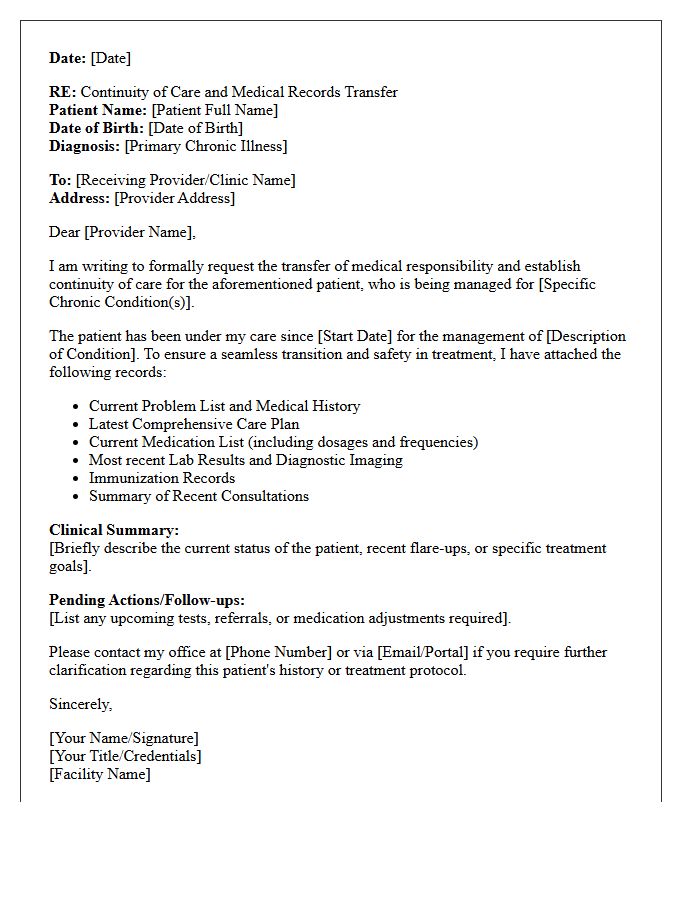
A Continuity of Care Letter is a vital medical document ensuring seamless transitions between healthcare providers. For patients with a chronic illness, this record summarizes your medical history, current medications, and ongoing treatment plans. It prevents gaps in clinical management and minimizes diagnostic errors during referrals. Providing this letter to new specialists ensures they understand your long-term health trajectory, enabling coordinated treatment and better outcomes. Always keep an updated copy to maintain patient safety and ensure that every member of your care team remains fully informed about your specific needs.
How can I request a copy of my chronic disease management records?
To request your chronic disease management records, you must submit a formal written request or a signed medical release form to your healthcare provider's medical records department. Most facilities allow you to submit this request via a secure patient portal, mail, or in-person at the clinic.
What information is typically included in chronic disease management documentation?
Chronic disease management records generally include your personalized care plan, longitudinal tracking of vital signs, lab results relevant to your condition (such as HbA1c for diabetes), medication history, specialist consultation notes, and documentation of self-management education sessions.
Is there a fee associated with obtaining my chronic illness treatment history?
While many providers offer digital access via patient portals for free, a reasonable cost-based fee may be charged for paper copies or records provided on physical media. These fees are regulated by state law and HIPAA guidelines to cover the costs of labor, copying, and postage.
How long does it take to process a request for chronic care coordination records?
Under HIPAA regulations, healthcare providers have up to 30 days to fulfill a request for medical records. However, many practices process requests for chronic disease documentation within 5 to 10 business days, especially if the records are stored electronically.
Can I authorize a third party or family member to access my chronic disease records?
Yes, you can authorize a third party, such as a caregiver or legal representative, to access your records by completing a HIPAA-compliant Authorization to Disclose Protected Health Information (PHI) form. This document must specify what information can be shared and the duration of the authorization.
Comments