A formal Request for Complete Medical Chart Audit Records is essential for ensuring clinical accuracy and compliance. This process helps healthcare providers identify documentation gaps and improve patient care standards through systematic reviews. Securing detailed reports allows for better financial oversight and legal protection. To streamline your documentation process, below are some ready to use templates.
Image cover: Professional Medical Chart Audit Request: Comprehensive Record Samples and Templates
Letter Samples List
- Internal Audit Request Letter for Complete Medical Chart Records
- Insurance Compliance Letter for Complete Medical Chart Audit Records
- Medicare Post-Payment Audit Letter for Complete Medical Chart Records
- Legal Counsel Request Letter for Complete Medical Clinic Chart Audit Records
- State Health Department Letter for Complete Medical Chart Audit Records
- Third-Party Billing Audit Letter for Complete Medical Chart Records
- Patient Representative Request Letter for Complete Medical Chart Audit Records
- Quality Assurance Review Letter for Complete Medical Chart Audit Records
- Medicaid Integrity Program Letter for Complete Medical Chart Records
- Clinic Peer Review Committee Letter for Complete Medical Chart Audit Records
- Risk Management Assessment Letter for Complete Medical Chart Records
- External Regulatory Compliance Letter for Complete Medical Chart Audit Records
Internal Audit Request Letter for Complete Medical Chart Records
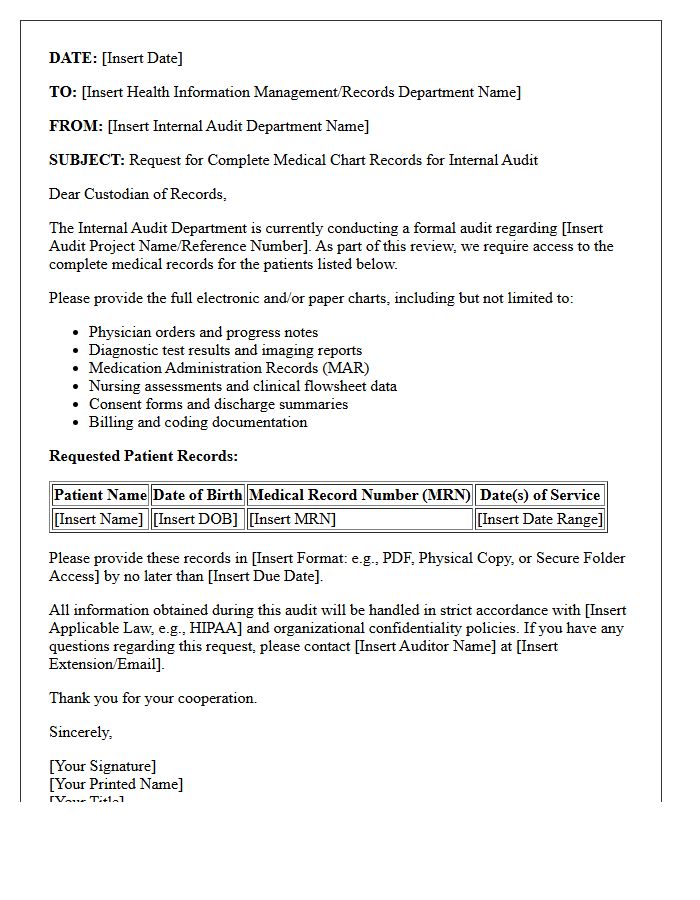
An Internal Audit Request Letter is a formal document used to secure complete medical chart records for quality assurance and compliance reviews. It must clearly specify the patient identifiers, required date ranges, and the exact clinical documentation needed to ensure a thorough evaluation. This request serves as a critical step in verifying documentation accuracy and identifying potential risks within healthcare operations. By maintaining a clear audit trail, organizations ensure regulatory compliance with HIPAA standards and improve the overall integrity of their internal medical reporting systems.
Insurance Compliance Letter for Complete Medical Chart Audit Records
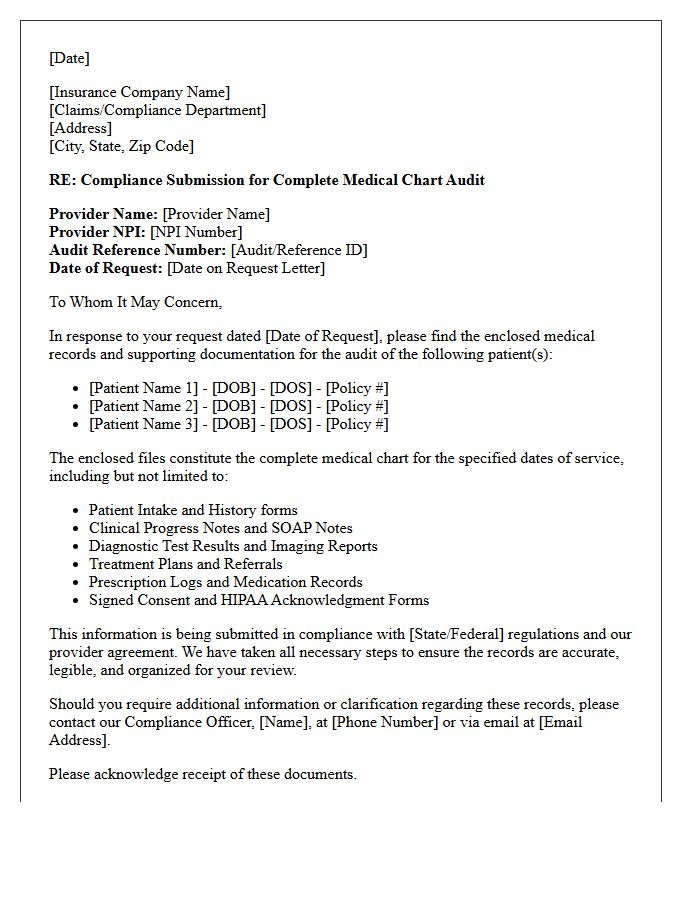
An Insurance Compliance Letter serves as a formal verification that a healthcare provider's documentation meets specific regulatory and payer standards. During a complete medical chart audit, insurers review clinical records to ensure accuracy, medical necessity, and coding integrity. Receiving this letter confirms that your practice adheres to legal mandates, reducing the risk of financial penalties or claim denials. It is essential to maintain organized, audit-ready records to prove policy adherence and safeguard professional reputation during federal or private insurance evaluations.
Medicare Post-Payment Audit Letter for Complete Medical Chart Records
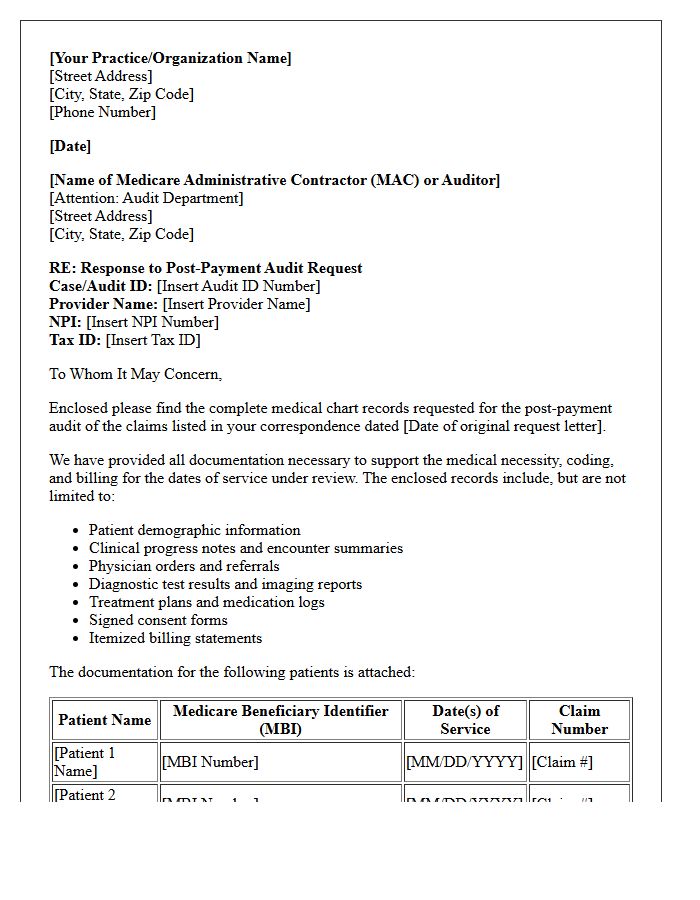
Receiving a Medicare Post-Payment Audit letter requires immediate action to verify billing accuracy. This request mandates submitting complete medical chart records, including physician notes, diagnostic results, and signed treatment plans. Failure to provide comprehensive documentation within the specified deadline can result in claim denials and mandatory repayment of funds. Ensure all entries are legible, chronologically ordered, and demonstrate medical necessity for the services rendered. Proactive compliance and thorough recordkeeping are essential to protecting your practice from financial penalties and ongoing regulatory scrutiny during federal oversight reviews.
Legal Counsel Request Letter for Complete Medical Clinic Chart Audit Records
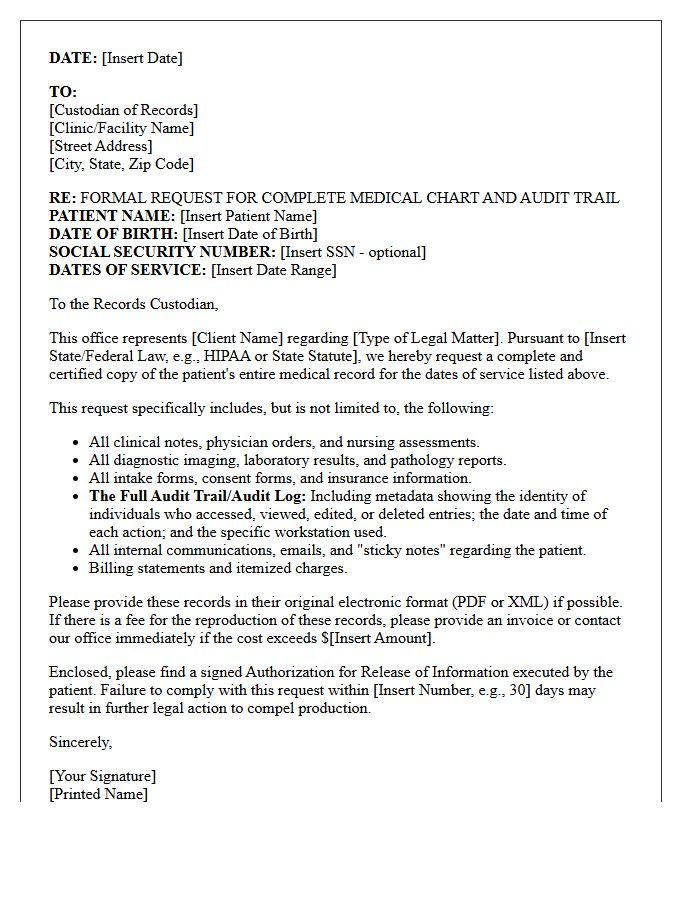
A formal Legal Counsel Request Letter is a critical document used to obtain complete medical clinic chart audit records for litigation or compliance reviews. This written demand must specify the patient's identity, required date ranges, and a valid HIPAA authorization to ensure data privacy. It is essential to request all comprehensive documentation, including electronic health records, clinician notes, and billing metadata. Obtaining the full, unredacted clinical audit trail allows legal teams to verify the accuracy of medical care and identify potential discrepancies in the healthcare provider's internal reporting systems.
State Health Department Letter for Complete Medical Chart Audit Records
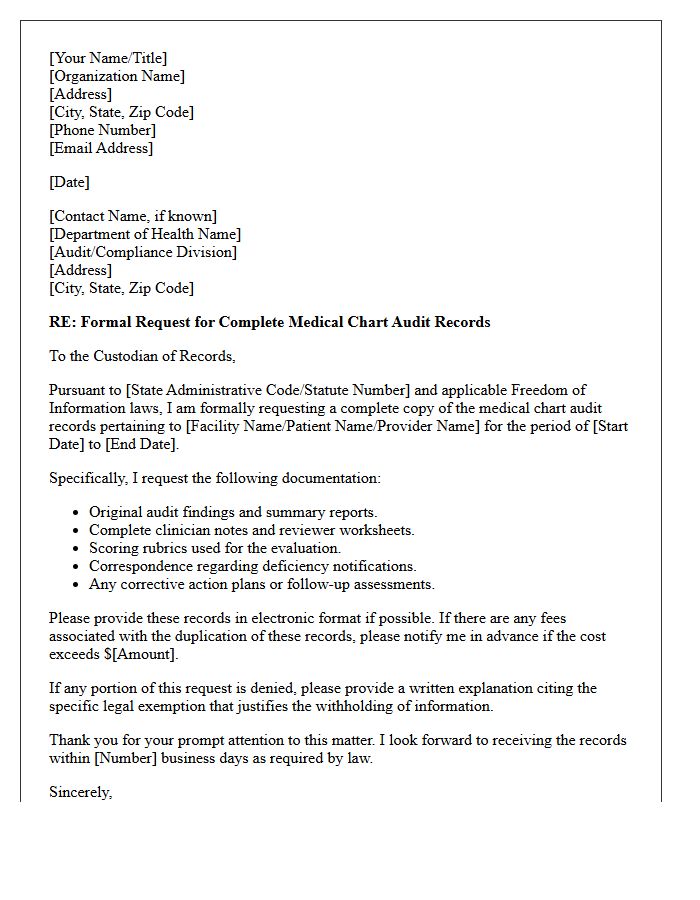
A State Health Department letter regarding a Complete Medical Chart Audit signifies a mandatory regulatory review of patient records. This formal notice requires healthcare facilities to provide comprehensive documentation, including treatment plans, progress notes, and billing data. The primary objective is to verify compliance with state healthcare standards, patient safety protocols, and accurate reporting practices. Facilities must ensure all entries are legible, signed, and organized sequentially. Timely cooperation is essential to maintain licensure and avoid potential penalties or legal action resulting from administrative discrepancies or incomplete medical histories discovered during the official inspection.
Third-Party Billing Audit Letter for Complete Medical Chart Records
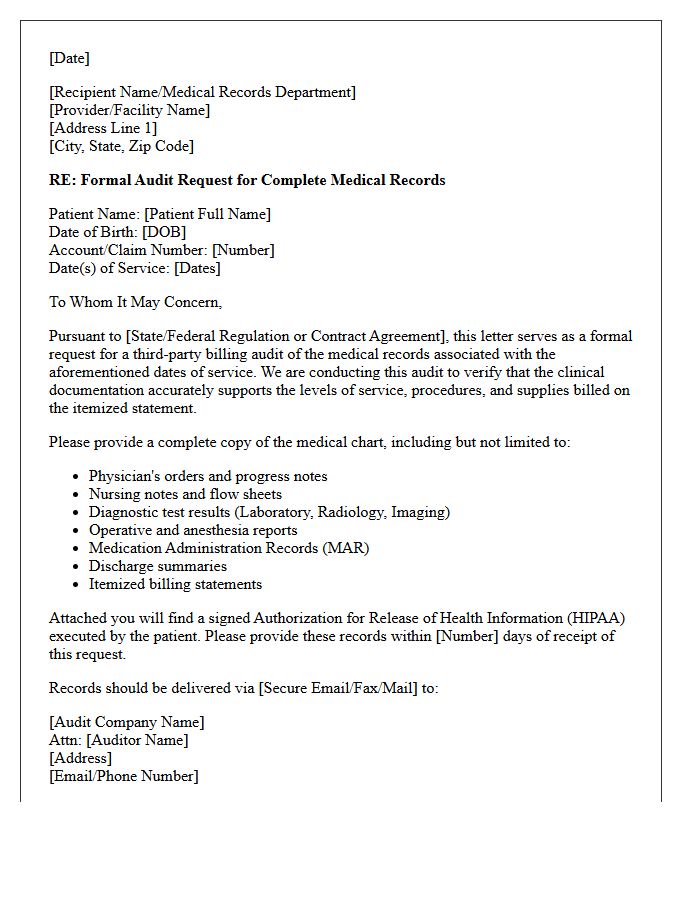
Receiving a Third-Party Billing Audit Letter indicates a formal review of your medical claims to ensure billing accuracy and compliance. Payers request Complete Medical Chart Records to verify that the documentation supports the specific codes billed. It is critical to provide legible, organized, and comprehensive notes, including physician signatures and diagnostic reports. Failure to submit requested information within the specified deadline can lead to claim denials, payment recoupments, or potential legal penalties. Proactive internal reviews and maintaining precise electronic health records are essential strategies to mitigate financial risks during these professional audits.
Patient Representative Request Letter for Complete Medical Chart Audit Records
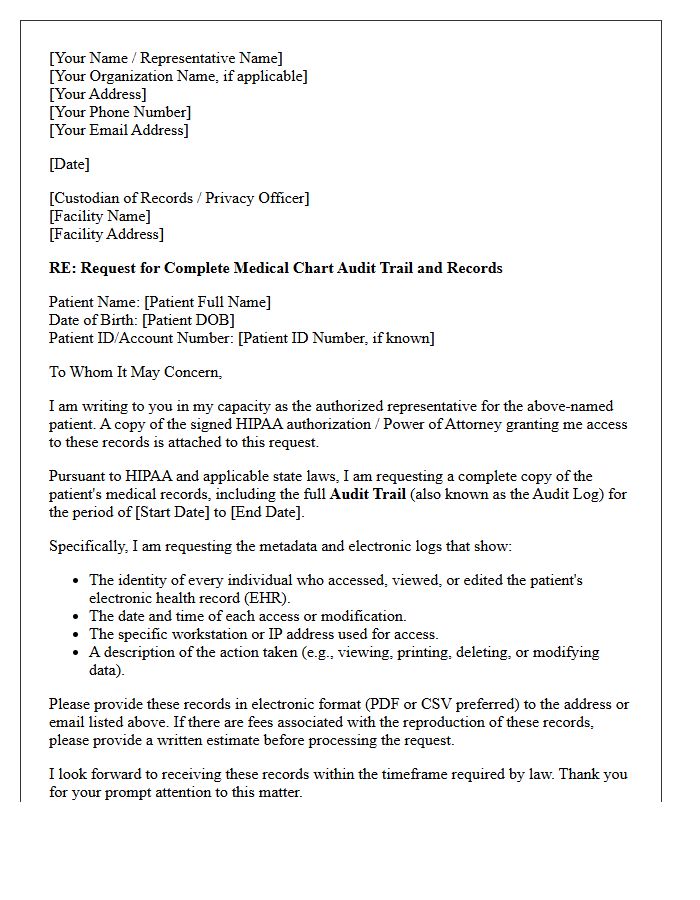
A Patient Representative Request Letter is a formal document used to authorize a third party to access a Complete Medical Chart Audit. This legal request ensures the disclosure of all health information, including clinician notes, diagnostic results, and billing records. To comply with HIPAA regulations, the letter must include the patient's full identification and a clear scope of the authorization. Providing this written consent allows representatives to review the entire medical history for legal, insurance, or personal care management purposes while maintaining strict patient privacy standards.
Quality Assurance Review Letter for Complete Medical Chart Audit Records
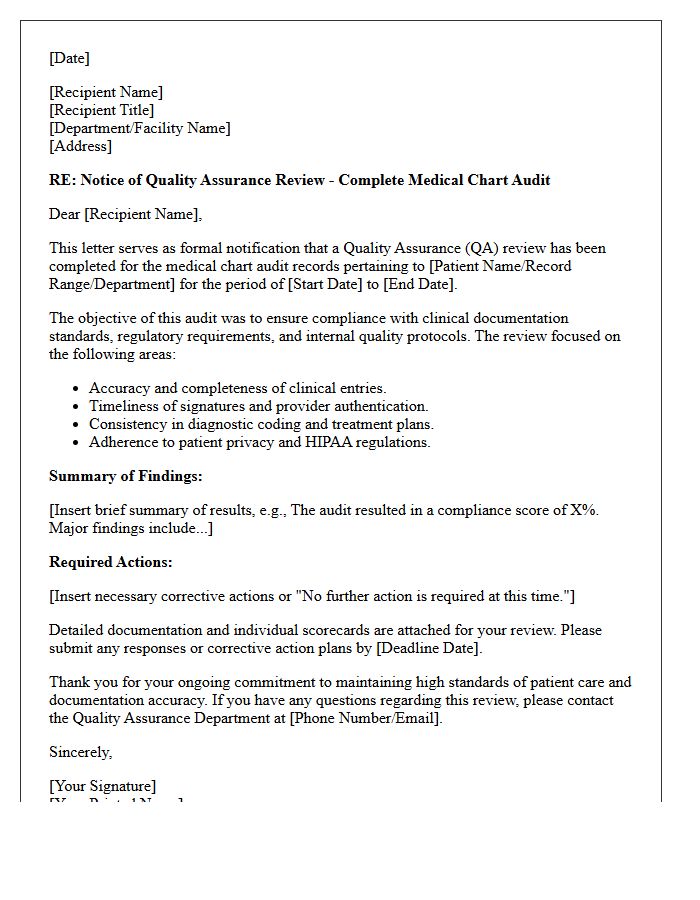
A Quality Assurance Review Letter serves as the formal validation of a Complete Medical Chart Audit. It documents the accuracy, compliance, and clinical necessity of patient records. This official summary identifies documentation gaps, coding errors, and adherence to regulatory standards. For healthcare providers, it is a critical tool for risk management and performance improvement, ensuring that healthcare data meets legal requirements. Receiving this letter confirms that the audit process is finalized, providing a transparent roadmap for corrective actions and maintaining the highest integrity of medical documentation protocols.
Medicaid Integrity Program Letter for Complete Medical Chart Records
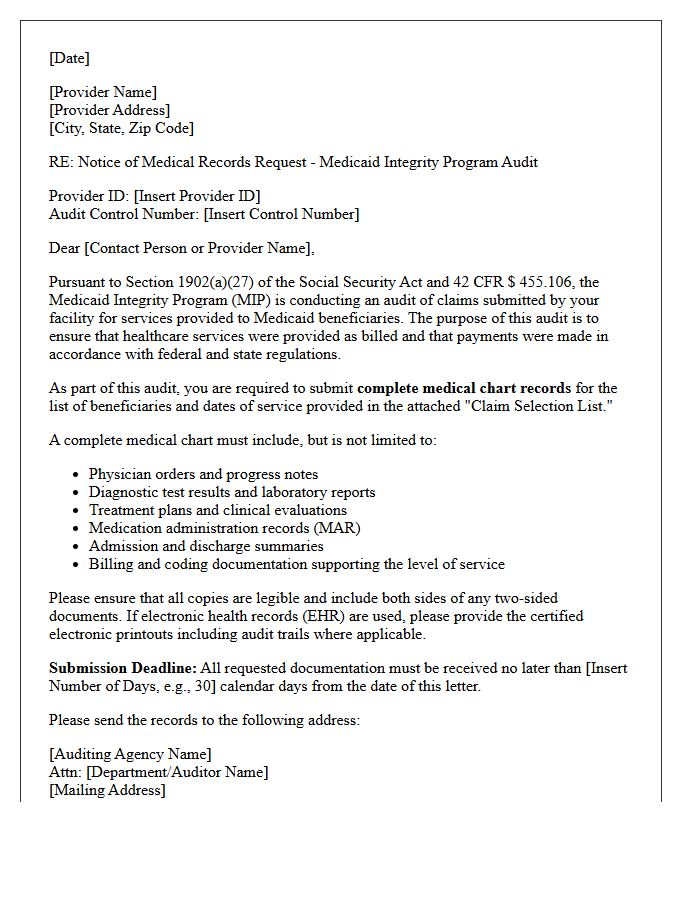
A Medicaid Integrity Program letter requesting complete medical chart records signifies a federal audit to verify payment accuracy and clinical necessity. Providers must submit comprehensive documentation, including progress notes, physician orders, and diagnostic results, within specified deadlines. Ensuring documentation integrity is vital, as missing or incomplete files can lead to significant financial recoupments, penalties, or allegations of fraud. Providers should conduct an immediate internal review to ensure all records align with Medicaid billing codes and strictly follow the submission instructions to maintain compliance and protect their practice from legal risks.
Clinic Peer Review Committee Letter for Complete Medical Chart Audit Records
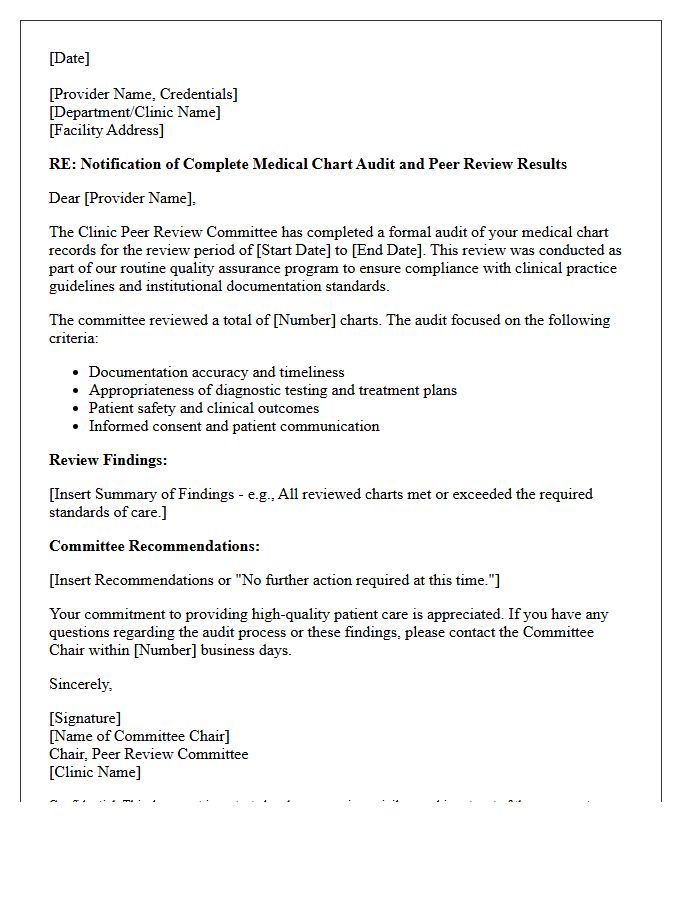
A Clinic Peer Review Committee Letter serves as a formal validation of a Complete Medical Chart Audit. This document confirms that a professional review committee has evaluated patient records for clinical accuracy, regulatory compliance, and quality of care. It is a critical component for credentialing and legal protection, ensuring that healthcare providers maintain rigorous standards. These letters summarize findings, identify areas for improvement, and document the systematic oversight necessary to mitigate risks and enhance patient safety protocols within a medical facility.
Risk Management Assessment Letter for Complete Medical Chart Records
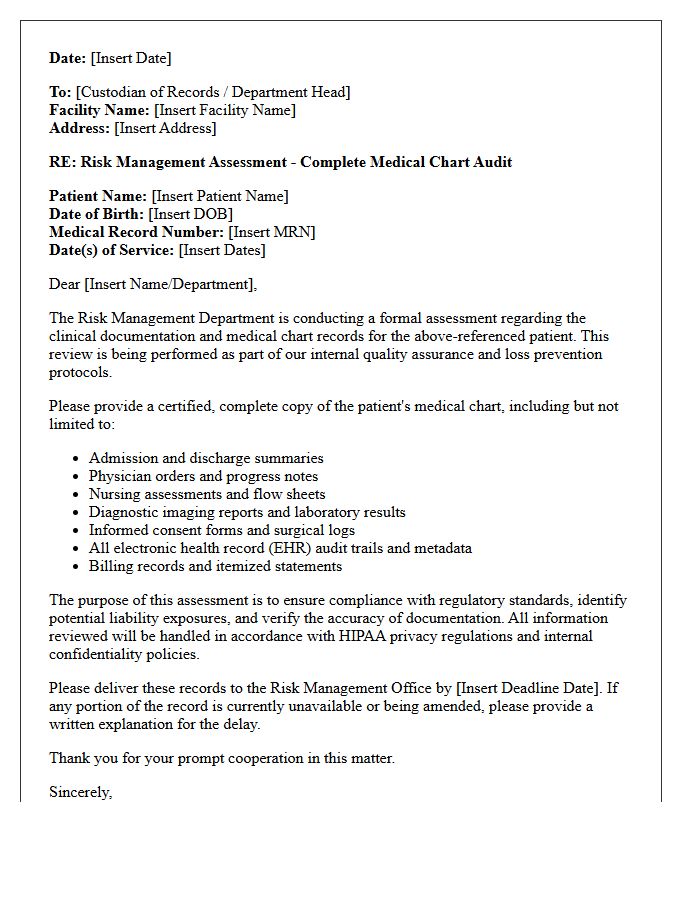
A Risk Management Assessment Letter is a critical document used to verify the integrity of complete medical chart records. It identifies potential liability gaps and ensuring regulatory compliance within clinical documentation. This assessment serves as a formal review to mitigate legal exposure by confirming that patient data is accurate, chronologically sound, and properly authenticated. By conducting this quality audit, healthcare providers can proactively address documentation deficiencies before they escalate into malpractice claims or audit failures, maintaining both patient safety and institutional security through precise record-keeping standards.
External Regulatory Compliance Letter for Complete Medical Chart Audit Records
An External Regulatory Compliance Letter serves as official certification that complete medical chart audit records meet mandatory healthcare standards. This document validates data integrity, patient privacy protection, and adherence to legal mandates like HIPAA. It provides essential legal protection and quality assurance for healthcare facilities during government inspections or insurance reviews. By confirming the accuracy and completeness of medical documentation, the letter mitigates audit risks, prevents financial penalties, and ensures that clinical practices align with current regulatory frameworks, maintaining the overall credibility of the healthcare organization's records management system.
How do I submit a formal request for a complete medical chart audit record?
To request a complete medical audit record, you must submit a written Authorization for Disclosure of Health Information to the Health Information Management (HIM) department. Ensure your request explicitly specifies "full audit logs" and "metadata" in addition to standard clinical documentation.
What information is included in a full medical chart audit trail?
A comprehensive audit trail includes timestamps for every entry, the identity of the individual accessing the record, specific actions taken (viewed, edited, or deleted), and the workstation used. This provides a chronological "who, what, and when" of your electronic protected health information (ePHI).
Is a patient legally entitled to view their medical record audit logs under HIPAA?
Yes, under the HIPAA Security Rule and HITECH Act, patients have the right to an "accounting of disclosures." While standard records contain clinical notes, audit logs are part of the designated record set that tracks how your information has been managed and accessed within an Electronic Health Record (EHR) system.
How long does a healthcare provider have to fulfill an audit record request?
Under federal HIPAA guidelines, providers generally have 30 days to fulfill a request for medical records, including audit trails. A one-time 30-day extension is permitted if the provider provides a written explanation for the delay and a projected completion date.
What is the difference between a standard medical record and an audit trail?
A standard medical record focuses on clinical care, such as diagnoses, lab results, and physician notes. An audit trail is a backend technical document that records the administrative history of the digital file, showing every instance the electronic chart was opened or modified by staff members.
Comments