Navigating the insurance process requires precision when seeking a Prior Authorization Extension for rehabilitative therapy. Extending care ensures patients receive uninterrupted physical, occupational, or speech therapy to reach recovery goals. Timely documentation and medical necessity justifications are essential for securing additional treatment visits from payers. To simplify your administrative workflow, below are some ready to use templates.
Image cover: Mastering the Art of Prior Authorization Extensions for Rehabilitative Therapy: Pro Templates and Samples
Letter Samples List
- Medical Clinic Letterhead and Contact Information
- Date of Letter Submission
- Health Insurance Payer Name and Address
- Patient Demographics and Insurance Policy Details
- Reference to Original Prior Authorization Number
- Subject Line for Prior Authorization Extension Request Letter
- Primary Diagnosis Codes and Medical History Summary
- Overview of Initial Rehabilitative Therapy Progress
- Current Functional Limitations and Objective Measurements
- Medical Necessity for Continued Rehabilitative Therapy Services
- Updated Treatment Plan and Specific Clinical Goals
- Requested Number of Additional Therapy Sessions
- Enclosed Supporting Clinical Documentation and Medical Records
- Attending Therapist and Medical Director Signatures
Medical Clinic Letterhead and Contact Information
A professional Medical Clinic Letterhead serves as a vital legal and branding document. It must clearly display the facility's official name, physical address, and direct contact information, including phone numbers and secure email. Accurate details ensure seamless patient communication and regulatory compliance. Essential elements often include the clinic logo, operating hours, and practitioner credentials. Maintaining a clean, organized layout fosters provider credibility and ensures that patients or referring physicians can easily reach the administrative staff for urgent inquiries or follow-up care instructions.
Date of Letter Submission
The Date of Letter Submission is the official day a document is formally delivered to its recipient. It serves as a legal timeline, establishing proof of communication for deadlines, contracts, or applications. Whether sent via email or post, ensuring an accurate date is critical for compliance and record-keeping. In formal correspondence, this date confirms when your obligations were met, protecting you against late penalties. Always verify the submission window to maintain professional accountability and ensure your message is recognized within the required effective period.
Health Insurance Payer Name and Address
When filing medical claims, the Health Insurance Payer Name and Address are critical for ensuring proper reimbursement. The Payer ID or name identifies the specific insurance company, while the claims mailing address directs the bill to the correct processing center. Always verify these details on the back of the member's insurance ID card, as they may differ from the corporate headquarters. Accuracy prevents claim denials, minimizes processing delays, and ensures that financial correspondence reaches the designated claims administrator promptly within the healthcare billing cycle.
Patient Demographics and Insurance Policy Details
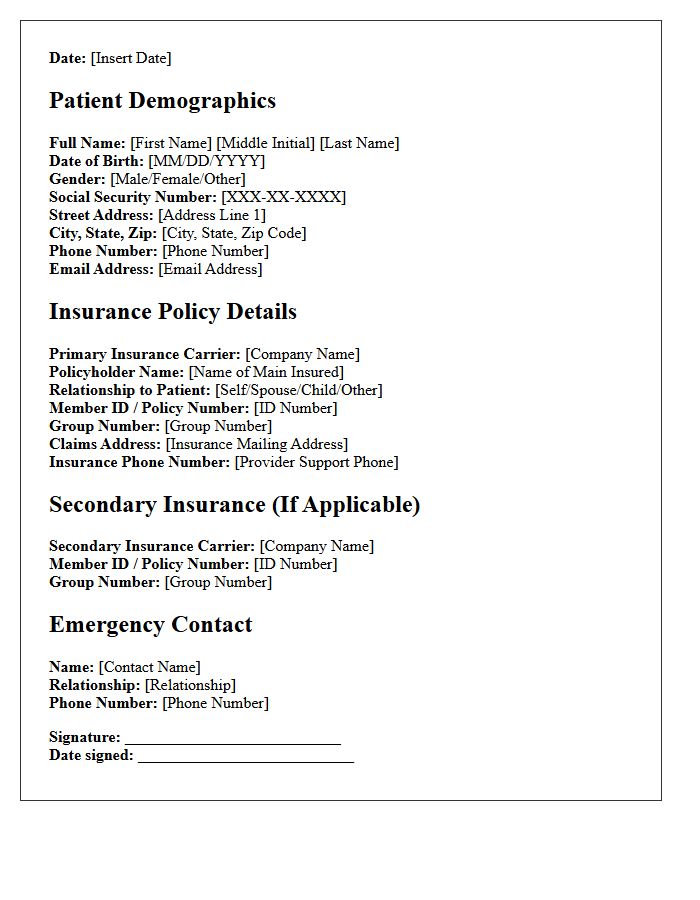
Accurate patient demographics and current insurance policy details are essential for seamless healthcare administration. Demographics include basic identifiers like full name, date of birth, and contact information, ensuring precise record matching. Simultaneously, verifying coverage specifics, such as group numbers, provider networks, and benefit limits, prevents claim denials and billing errors. Collecting this data during intake streamlines the revenue cycle management process, reduces administrative delays, and ensures patients receive timely care without unexpected financial burdens. Maintaining updated records is the foundation of efficient clinical workflows and effective communication.
Reference to Original Prior Authorization Number
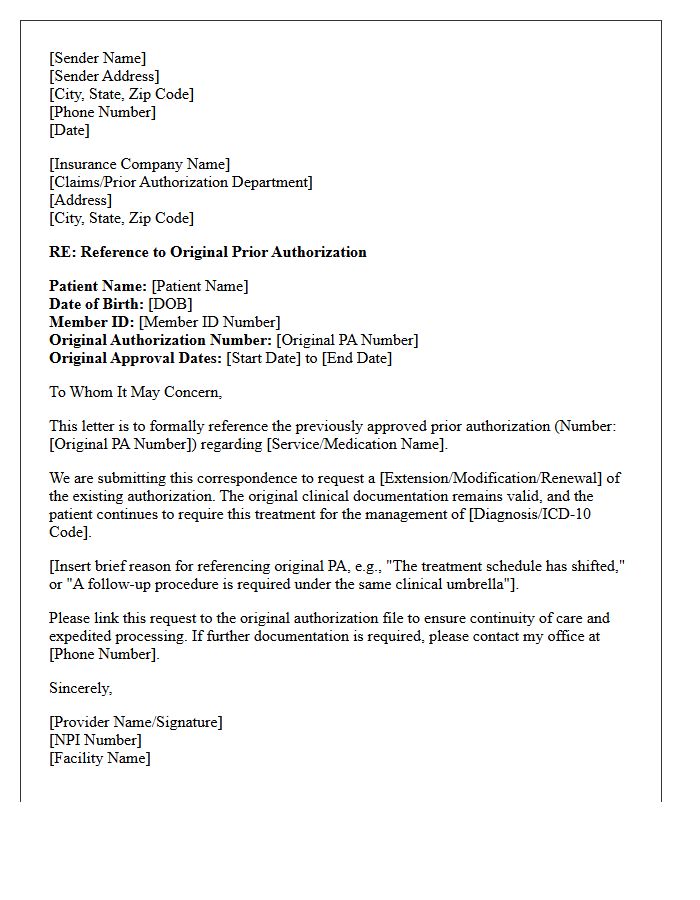
When submitting a Prior Authorization renewal or appeal, including the Original Prior Authorization Number is essential. This reference links current requests to previous medical necessity approvals, ensuring continuity of care and faster processing. Claims adjusters use this unique identifier to track the authorization history, minimize administrative delays, and prevent potential denials. Always double-check that the reference number matches exactly as issued by the insurance provider to maintain an accurate and auditable medical record within the billing cycle.
Subject Line for Prior Authorization Extension Request Letter
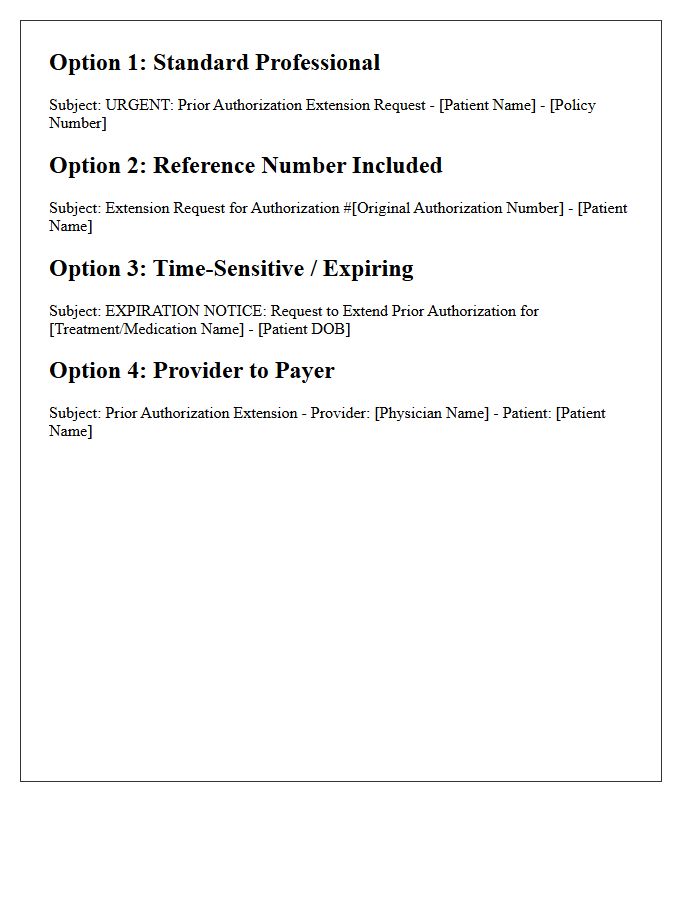
When drafting a subject line for a Prior Authorization Extension Request, clarity is vital for rapid processing. You must include the patient's full name, date of birth, and the specific authorization reference number. Clearly state the purpose by using phrases like "Urgent Extension Request" to ensure the insurance reviewer identifies the timeline immediately. Including the provider's NPI number can also expedite the lookup process. A concise, professional subject line prevents administrative delays, ensuring uninterrupted patient care and timely medical necessity re-evaluation by the payer's utilization management department.
Primary Diagnosis Codes and Medical History Summary
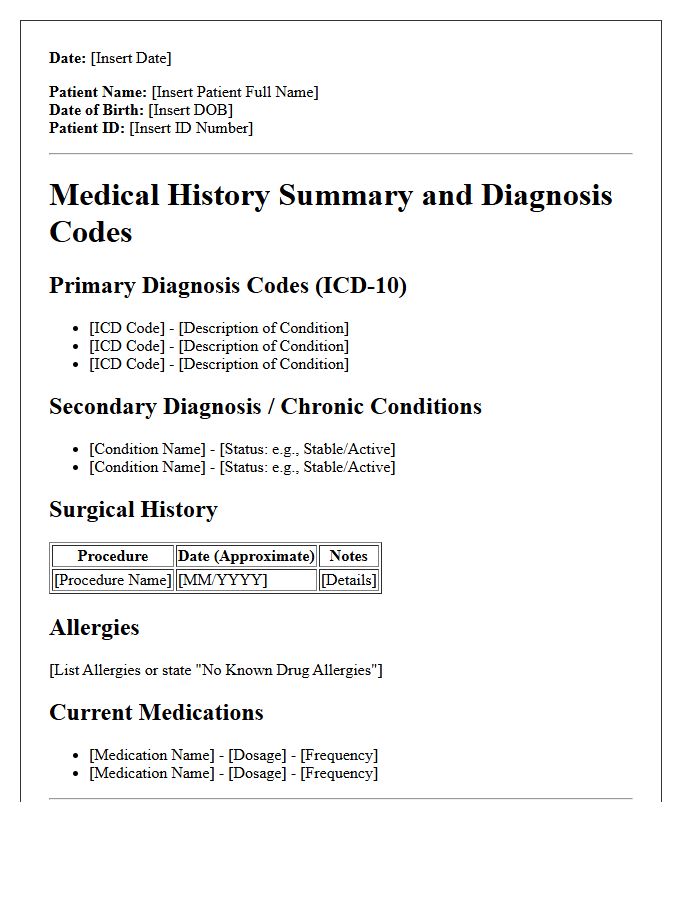
A Primary Diagnosis Code is the fundamental alphanumeric identifier, typically using ICD-10 standards, that justifies the main reason for a patient's medical encounter. It is essential for accurate insurance reimbursement and clinical tracking. This code works alongside a Medical History Summary, which provides a comprehensive overview of past illnesses, surgeries, and chronic conditions. Together, these elements ensure continuity of care by giving healthcare providers a clear clinical picture, reducing errors, and documenting the patient's longitudinal health status for effective long-term treatment planning.
Overview of Initial Rehabilitative Therapy Progress
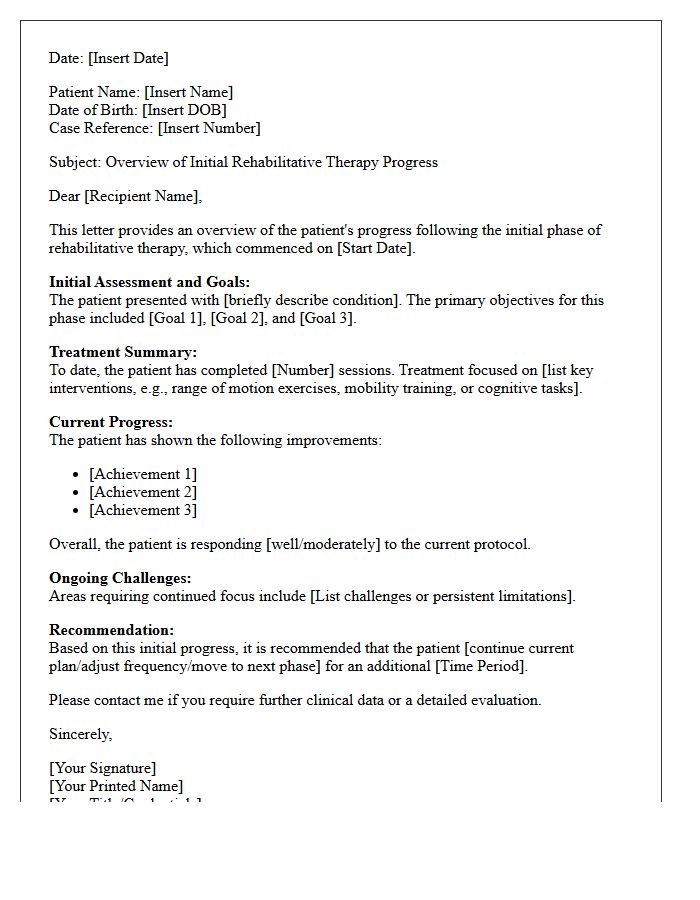
Initial rehabilitative therapy focuses on establishing a functional baseline and setting personalized recovery goals. During this phase, therapists assess mobility, strength, and range of motion to design a specific treatment plan. Early progress is often measured by the patient's ability to perform activities of daily living and manage pain effectively. Consistency in performing prescribed exercises is the most critical factor for long-term success. Monitoring these early milestones ensures the rehabilitation process remains adaptive, allowing for timely adjustments to interventions and improving overall clinical outcomes during the healing journey.
Current Functional Limitations and Objective Measurements
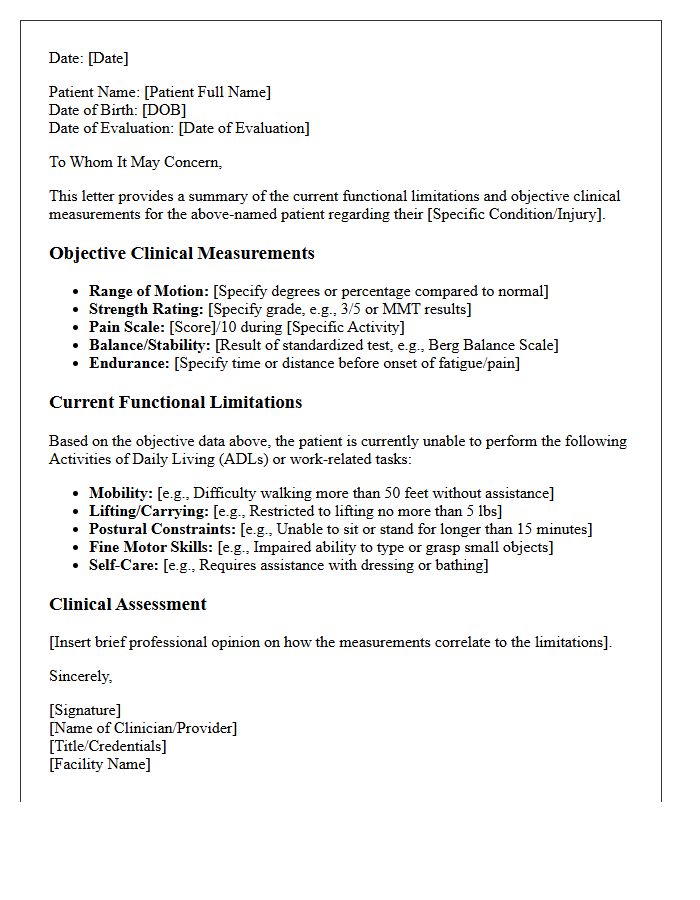
Modern clinical assessments require objective measurements to accurately track patient progress and justify medical necessity. Relying solely on subjective self-reporting often leads to data gaps. Clinicians must identify specific functional limitations, such as reduced range of motion or diminished grip strength, using standardized tools like goniometers or dynamometers. These quantifiable metrics transform abstract physical impairments into actionable data. By documenting precise baseline values and incremental changes, providers ensure evidence-based treatment plans while meeting strict regulatory requirements for functional reporting and reimbursement accuracy.
Medical Necessity for Continued Rehabilitative Therapy Services
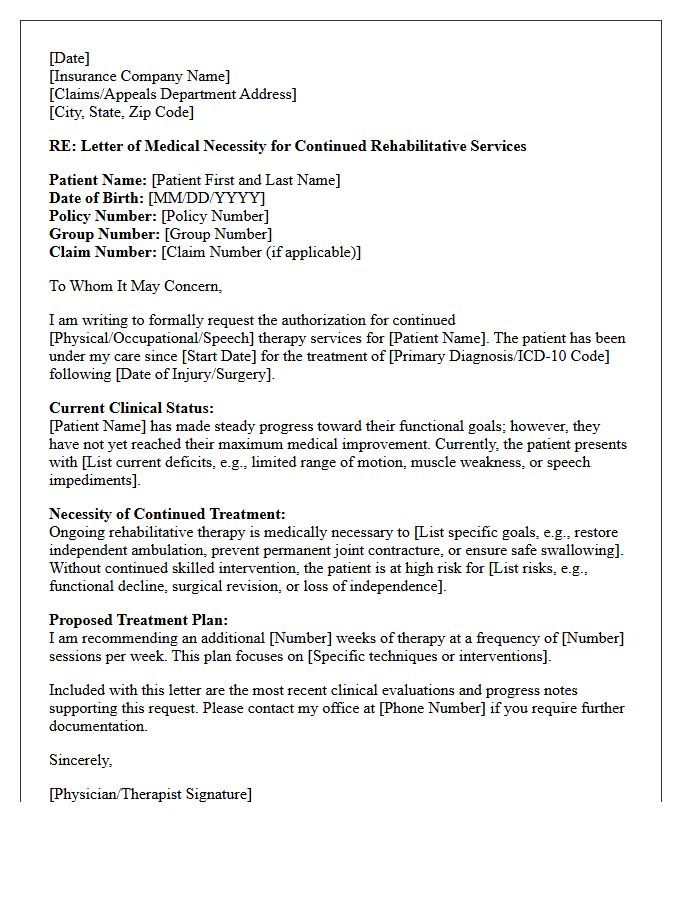
In healthcare, medical necessity is the fundamental requirement for insurance coverage of ongoing care. For continued rehabilitative therapy, providers must document that the patient shows measurable functional progress or requires a skilled therapist to maintain current abilities and prevent clinical deterioration. Documentation must clearly justify that services are clinically appropriate, effective, and specifically tailored to the patient's diagnosis. If the therapy becomes maintenance-based without a skilled need, or if the patient reaches a plateau without further potential for improvement, the services may no longer be deemed medically necessary for reimbursement purposes.
Updated Treatment Plan and Specific Clinical Goals
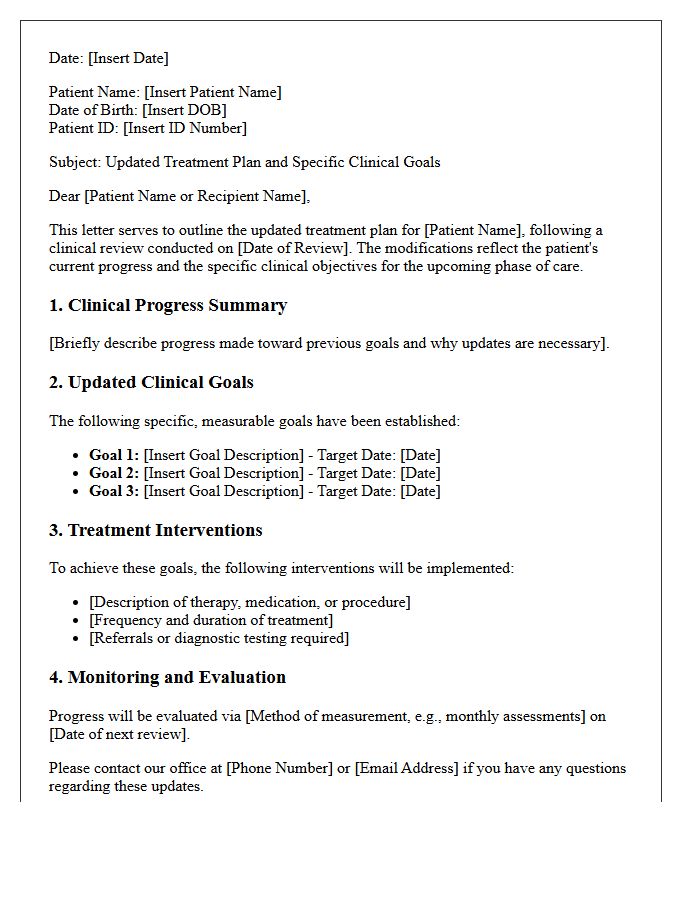
An Updated Treatment Plan is essential for documenting a patient's evolving recovery journey. It transitions from general assessments to Specific Clinical Goals, which must be measurable, time-bound, and evidence-based. These updates ensure that therapeutic interventions remain aligned with current progress, addressing new challenges or stabilizing symptoms. By refining objectives regularly, clinicians provide a roadmap for targeted outcomes, improving accountability and the overall quality of care. Clear documentation of these adjustments facilitates better communication among the healthcare team and ensures the most effective treatment strategies are consistently applied.
Requested Number of Additional Therapy Sessions
When seeking a Requested Number of Additional Therapy Sessions, clinical necessity is the primary requirement. Insurance providers typically evaluate medical necessity through progress reports and updated treatment plans. It is essential to demonstrate how further sessions will achieve specific health goals. Clear documentation of functional improvements and remaining symptoms helps justify the extension. Patients should discuss authorization timelines with their providers early to avoid treatment interruptions. Ensuring all paperwork accurately reflects the need for ongoing care increases the likelihood of approval for extended mental health support.
Enclosed Supporting Clinical Documentation and Medical Records
When submitting claims, providing Enclosed Supporting Clinical Documentation is essential to verify medical necessity and ensure accurate reimbursement. These records must include comprehensive progress notes, diagnostic results, and treatment plans that align with billed services. Proper documentation serves as a legal bridge between patient care and financial validation, reducing the risk of denials or audits. Always ensure that medical records are legible, complete, and strictly adhere to HIPAA privacy standards to maintain patient confidentiality while facilitating a seamless claims adjudication process.
Attending Therapist and Medical Director Signatures
In clinical documentation, the Attending Therapist and Medical Director signatures are essential for legal compliance and reimbursement. The therapist confirms the direct delivery of evidence-based care, while the Medical Director provides oversight, validating the medical necessity of the treatment plan. Together, these signatures ensure that the services meet professional standards and insurance requirements. Missing or incomplete signatures can lead to audit failures and claim denials, making authenticated documentation a critical component of healthcare accountability and patient safety protocols.
How do I request an extension for prior authorization of rehabilitative therapy services?
To request an extension, providers must submit a clinical update or re-evaluation report before the current authorization expires. This submission should include progress notes, updated functional goals, and a justification for the medical necessity of continued treatment.
When should a prior authorization extension request be submitted?
Extension requests should typically be submitted 7 to 10 business days prior to the expiration date of the existing authorization. Late submissions may result in a gap in covered services or administrative denial.
What clinical documentation is required for a therapy authorization extension?
Required documentation includes the current plan of care, objective measurements of progress (such as standardized test scores), documentation of patient compliance, and a clear explanation of why the patient has not yet met their discharge goals.
Can I request additional therapy visits if the initial authorization has expired?
If the authorization has already expired, most payers require a new initial authorization request rather than an extension. It is critical to monitor authorization end dates to ensure continuity of care through the extension process.
What are the common reasons for denial of a rehabilitative therapy extension?
Common reasons for denial include a lack of documented functional improvement, failure to update the plan of care, missing objective data, or the services being deemed "maintenance therapy" rather than restorative rehabilitative care.
Comments