Navigating the Prior Authorization Request process is essential for securing coverage for intensive inpatient rehabilitation. This guide outlines necessary medical necessity documentation, clinical criteria, and provider requirements to ensure timely patient access to specialized recovery services. Streamline your clinical workflow and reduce claim denials by following industry standards for authorization submissions. Below are some ready to use template.
Image cover: Streamlining Your Inpatient Rehab Referrals: Professional Prior Authorization Templates and Samples
Letter Samples List
- Medical Clinic Letterhead Information
- Date of Letter Submission
- Insurance Payer Contact Details
- Patient Demographics and Insurance Information
- Prior Authorization Request Letter Subject Line
- Formal Letter Salutation
- Patient Primary Diagnosis and Medical History
- Clinical Justification for Inpatient Rehabilitation Admission
- Documentation of Failed Outpatient Treatments
- Expected Inpatient Rehabilitation Goals
- Proposed Treatment Plan and Duration
- Attending Physician Letter Signature and Credentials
- Enclosed Supporting Clinical Documentation
Medical Clinic Letterhead Information
A professional medical clinic letterhead must prioritize clarity and legal compliance. It should prominently feature the official practice name and a high-resolution logo to establish brand identity. Essential contact details include the physical address, phone number, and a secure fax line. To ensure medical credibility, always list the practitioners' names with their respective credentials. Including the clinic's website and registration numbers ensures patients and regulatory bodies can verify the facility. A clean, organized layout conveys trustworthiness, ensuring that all correspondence remains professional, legible, and legally sound for formal healthcare communication.
Date of Letter Submission
The Date of Letter Submission is the official day a document is formally delivered to its recipient. It serves as a legal timestamp, establishing deadlines and tracking compliance for formal applications or notices. In professional correspondence, this date confirms when your message was sent, which is vital for statutory timeframes and organizational records. Ensuring this date is accurate prevents administrative delays and provides essential proof of delivery in case of future disputes or verification needs.
Insurance Payer Contact Details
Accurate Insurance Payer Contact Details are essential for streamlining medical billing and ensuring timely claim reimbursements. Providers must maintain a verified directory including provider relations phone numbers, dedicated claims submission addresses, and specific electronic payer IDs. Having direct access to prior authorization departments prevents service delays and reduces claim denials. Since contact information frequently changes due to mergers or policy updates, regular credentialing audits are necessary to maintain data integrity and facilitate effective communication between healthcare facilities and insurance carriers.
Patient Demographics and Insurance Information
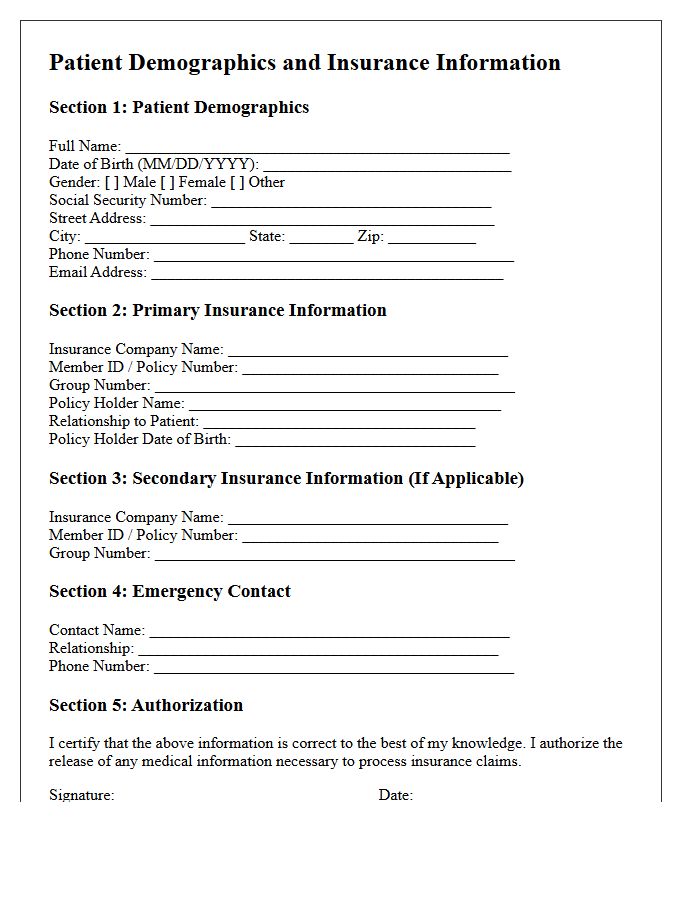
Accurate Patient Demographics and insurance details are vital for seamless healthcare delivery and billing. Demographics include essential identifiers like full name, date of birth, and contact information to ensure patient safety and reduce medical errors. Verifying Insurance Information, such as policy numbers and coverage limits, prevents claim denials and ensures financial transparency. Maintaining precise, updated records streamlines administrative workflows, facilitates effective communication between providers, and guarantees that individuals receive the correct treatment while maximizing their entitled benefits through precise identity verification.
Prior Authorization Request Letter Subject Line
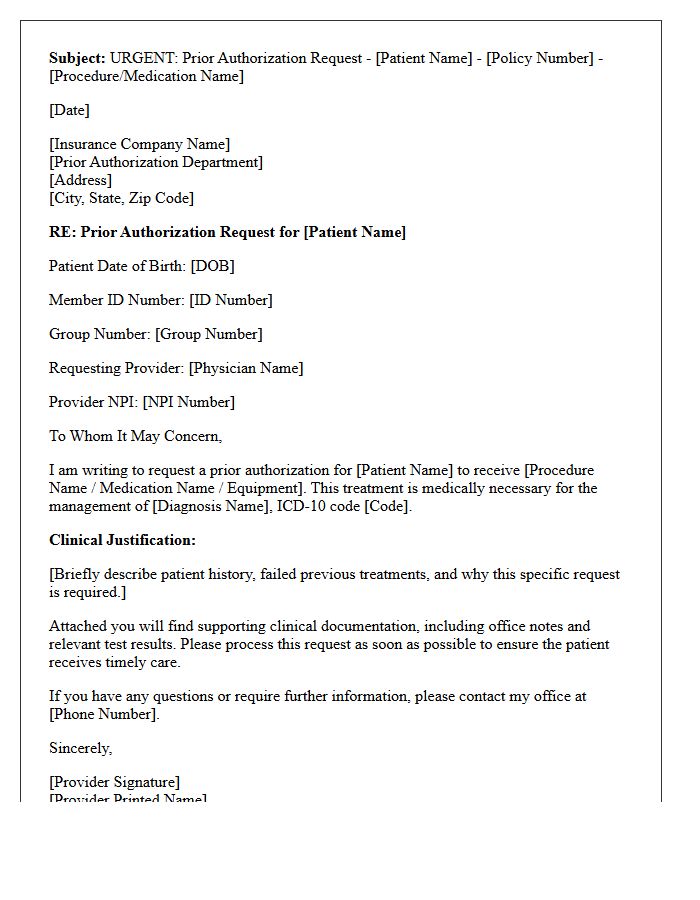
A Prior Authorization Request Letter Subject Line must be clear and concise to ensure timely insurance review. It is essential to include the Patient's Full Name, Date of Birth, and Member ID number. Additionally, clearly state the Urgency Level, such as "STAT" or "Urgent," alongside the specific Medical Procedure or medication requested. Including the Provider's NPI number can further expedite identification. A well-structured subject line minimizes administrative delays, helping healthcare providers secure necessary approvals for patient care efficiently while preventing the request from being overlooked by payers.
Formal Letter Salutation
When writing a formal letter, the salutation sets the professional tone. If the recipient's name is unknown, use "Dear Sir or Madam" or "To Whom It May Concern". However, addressing the person by their title and surname, such as "Dear Dr. Smith," is preferred for a personalized touch. Always follow the greeting with a colon or comma to maintain proper business etiquette. Choosing the correct salutation demonstrates respect and ensures your correspondence is received seriously by the intended audience.
Patient Primary Diagnosis and Medical History
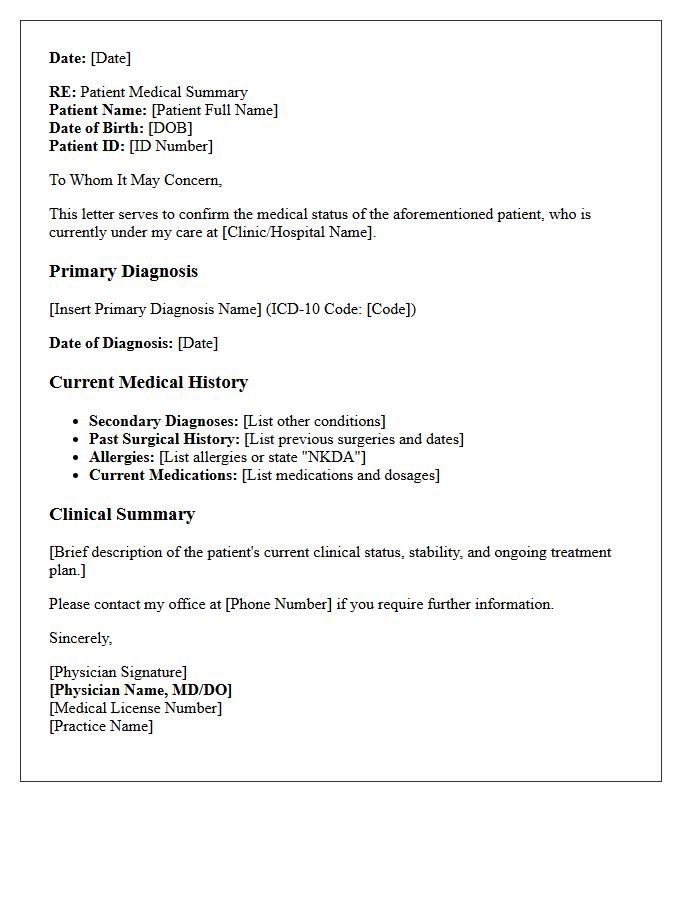
Understanding the Primary Diagnosis is essential as it identifies the main condition requiring immediate clinical intervention. This core diagnosis guides the current treatment plan and resource allocation. Simultaneously, a comprehensive Medical History provides vital context, documenting past illnesses, chronic conditions, and previous surgeries. Combining these elements allows healthcare providers to anticipate potential complications, avoid adverse drug interactions, and ensure holistic care. Accurate documentation of both clinical status and historical health data is the foundation for effective medical decision-making and improved patient outcomes.
Clinical Justification for Inpatient Rehabilitation Admission
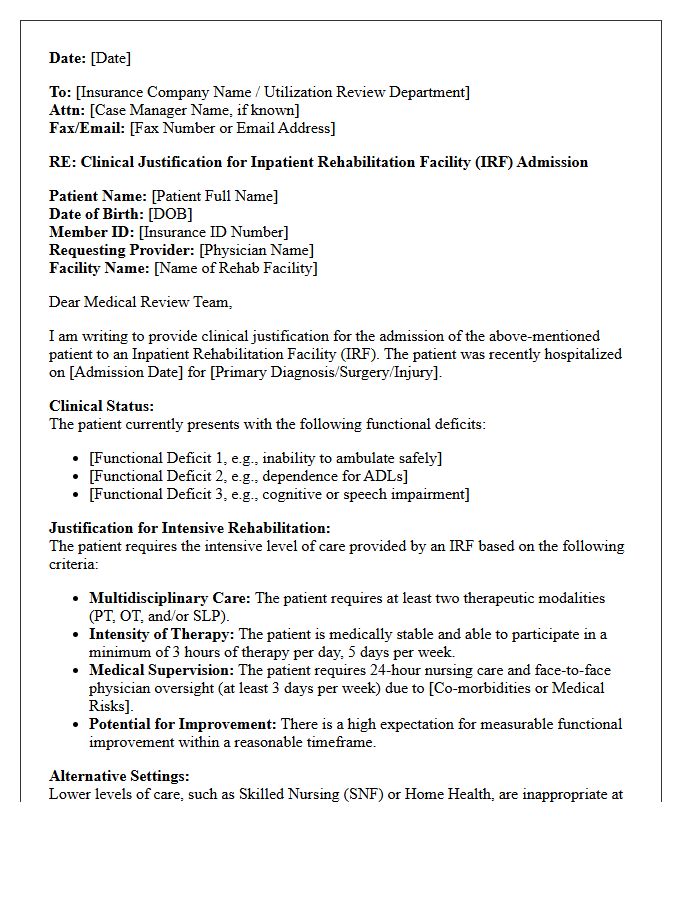
Clinical justification for inpatient rehabilitation requires documented evidence that a patient necessitates intensive therapy consisting of at least two disciplines. Medical necessity is established when a patient's condition is complex enough to require 24-hour rehabilitation nursing and face-to-face supervision by a specialized physician. The patient must demonstrate the physical and cognitive potential to participate in a minimum of three hours of therapy daily. Ultimately, the interdisciplinary team must prove that these coordinated services are essential for achieving significant functional improvement that cannot be safely managed in a lower level of care.
Documentation of Failed Outpatient Treatments
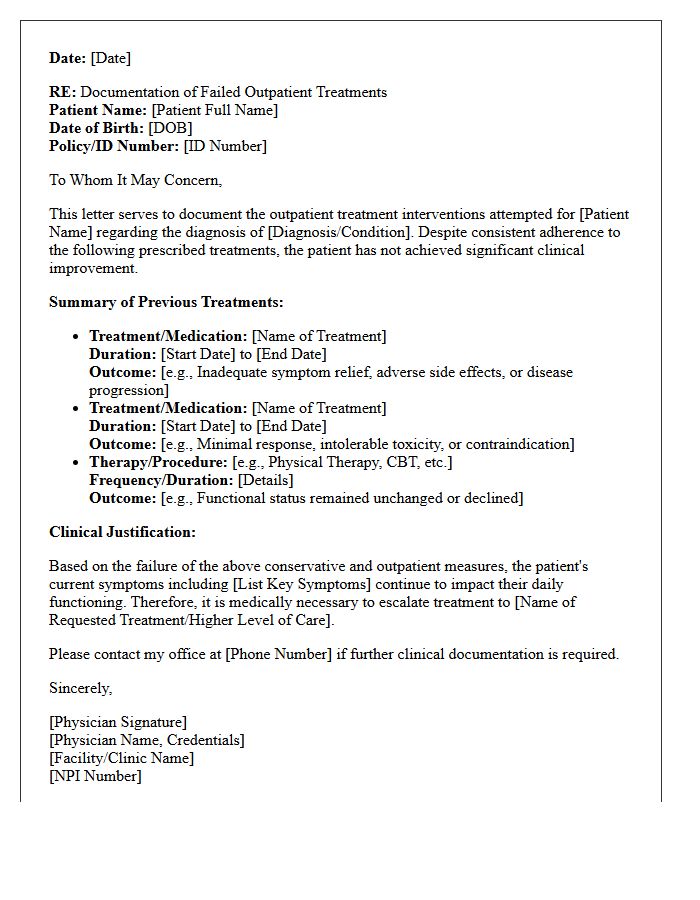
Precise documentation of failed outpatient treatments is essential for clinical continuity and insurance justification. Providers must record specific medication trials, dosages, and durations to prove medical necessity for advanced interventions. Clearly detailing adverse reactions or a lack of therapeutic response ensures a comprehensive patient history. This practice facilitates step therapy overrides and supports the transition to more intensive care levels, ultimately improving long-term health outcomes and ensuring regulatory compliance within the healthcare system.
Expected Inpatient Rehabilitation Goals
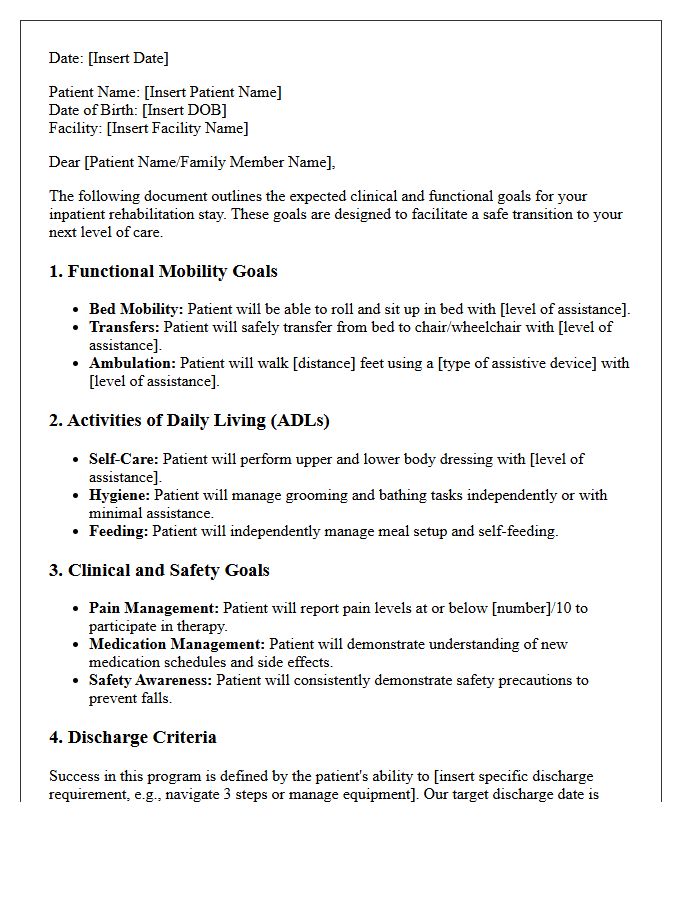
The primary aim of inpatient rehabilitation is to restore functional independence through intensive therapies. Patients work toward personalized mobility milestones, such as walking or transferring safely, to facilitate a secure return home. Clinicians focus on improving activities of daily living, including dressing and feeding, while managing medical stability. Achieving these rehabilitation goals requires active participation in physical, occupational, and speech therapy sessions. Ultimately, the program strives to enhance the patient's quality of life by reducing physical limitations and preparing caregivers for necessary long-term support and follow-up care transitions.
Proposed Treatment Plan and Duration
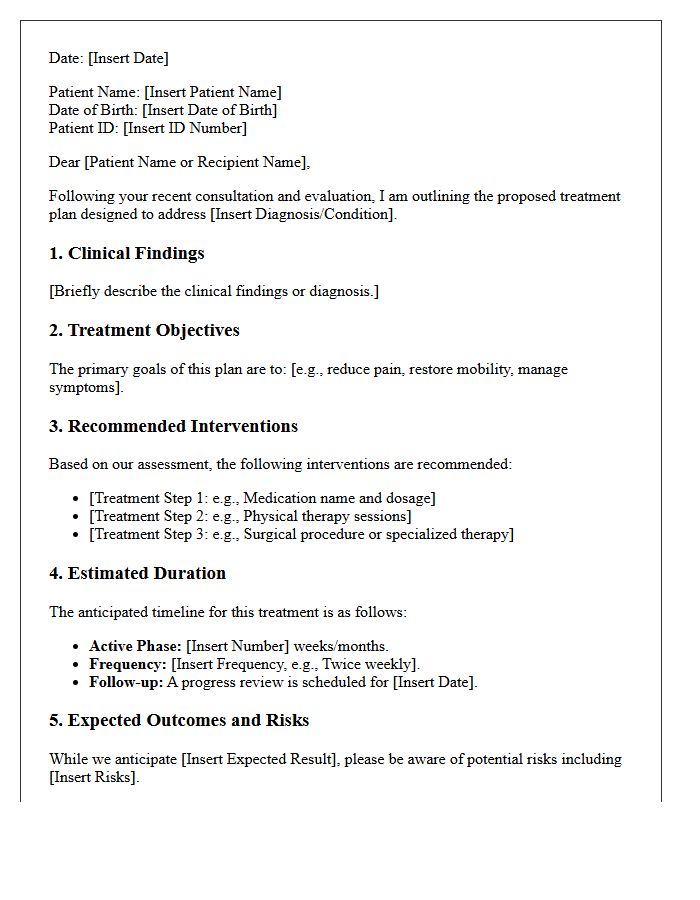
A proposed treatment plan outlines the specific therapeutic interventions tailored to a patient's diagnosis. It serves as a clinical roadmap, detailing the clinical objectives, medication dosages, and necessary procedures. Understanding the duration is vital, as it establishes the expected timeframe for recovery and the frequency of follow-up visits. Patients must review these documents to ensure informed consent and adherence. Clear communication regarding milestones helps manage expectations and improves health outcomes by aligning the provider's strategy with the patient's lifestyle and long-term wellness goals.
Attending Physician Letter Signature and Credentials
An official Attending Physician Letter must feature a wet or high-resolution electronic signature to ensure legal authenticity. To meet professional medical standards, the practitioner must clearly list their credentials, such as MD or DO, alongside their board certifications and state license number. This documentation verifies the provider's authority to render a diagnosis or recommendation. Omitting these formal identifiers can lead to the immediate rejection of insurance claims, legal affidavits, or clinical referrals. Always verify that the contact information matches the registered medical facility letterhead for institutional verification.
Enclosed Supporting Clinical Documentation
Enclosed supporting clinical documentation is essential for medical necessity verification. It includes detailed patient records, lab results, and physician notes submitted alongside insurance claims. Providing comprehensive evidence ensures accurate claim adjudication and reduces the risk of denials or delays. This documentation bridges the gap between diagnostic codes and actual patient care, offering a clear clinical picture for reimbursement approval. Maintaining organized, precise, and relevant data is the most effective way to streamline the healthcare billing process and support professional clinical decisions.
What information is required for a Prior Authorization Request for Inpatient Rehabilitation?
A complete request must include the patient's current clinical status, functional deficits, the specific medical necessity for 24-hour nursing care, and a physician-signed plan of care outlining the required multidisciplinary therapies (PT, OT, speech, or prosthetics/orthotics).
What are the clinical criteria for approving an Inpatient Rehabilitation Facility (IRF) admission?
Approval is based on the patient's need for intensive rehabilitation (typically 3 hours of therapy per day, 5 days a week), the requirement for frequent face-to-face physician supervision, and the documented potential for significant measurable functional improvement within a reasonable timeframe.
How long does the prior authorization process take for inpatient rehab?
Standard authorization requests are typically processed within 2 to 5 business days; however, "urgent" or "expedited" requests for patients currently in an acute care setting are generally reviewed within 24 to 72 hours to ensure a seamless transition of care.
Can an Inpatient Rehabilitation request be denied if the patient can tolerate a Skilled Nursing Facility (SNF)?
Yes. If the clinical documentation suggests the patient does not require the intensive 3-hour therapy daily or the high level of medical supervision provided in an IRF, the request may be redirected to a lower level of care, such as a Skilled Nursing Facility or outpatient rehabilitation.
How can a provider appeal a denied Prior Authorization for rehabilitation services?
Providers can initiate an appeal by submitting a formal request for reconsideration, which often includes a "Peer-to-Peer" review between the treating physician and the insurance medical director to discuss additional clinical nuances not captured in the initial documentation.
Comments